Department of Critical Care Medicine, State Key Laboratory of Complex Severe and Rare Diseases, Peking Union Medical College Hospital, Peking Union Medical College & Chinese Academy of Medical Sciences, 1 Shuaifuyuan, Dongcheng District, Beijing, 100730, China.
Digital Health China Technologies Co. Ltd., Floor 19, China Technology Exchange Building, 66 West Beisihuan Road, Haidian District, Beijing, 100080, China.
BMC Med Inform Decis Mak. 2021 Jul 30;21(Suppl 2):79. doi: 10.1186/s12911-021-01452-7.
Analgesia and sedation therapy are commonly used for critically ill patients, especially mechanically ventilated patients. From the initial nonsedation programs to deep sedation and then to on-demand sedation, the understanding of sedation therapy continues to deepen. However, according to different patient's condition, understanding the individual patient's depth of sedation needs remains unclear.
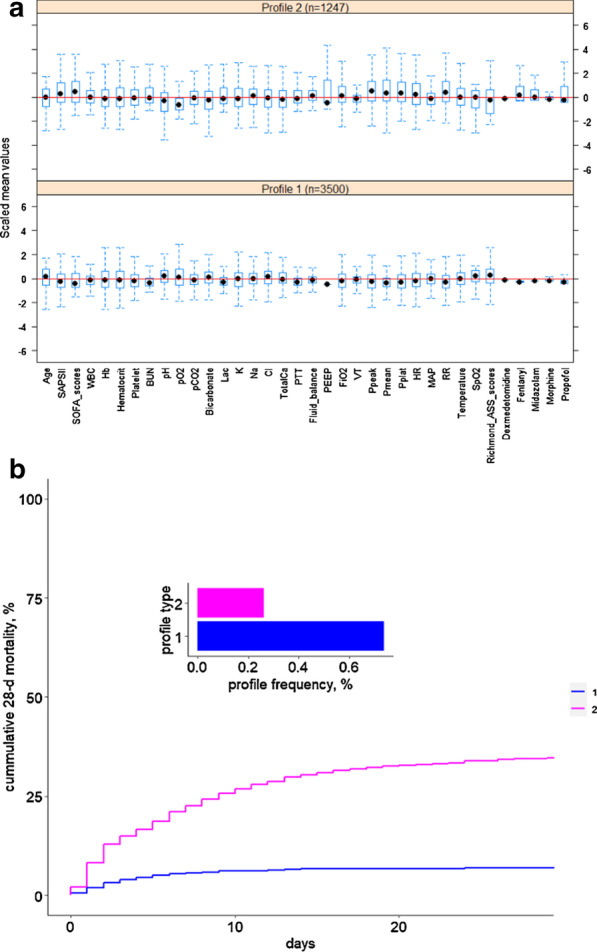
The public open source critical illness database Medical Information Mart for Intensive Care III was used in this study. Latent profile analysis was used as a clustering method to classify mechanically ventilated patients based on 36 variables. Principal component analysis dimensionality reduction was used to select the most influential variables. The ROC curve was used to evaluate the classification accuracy of the model.
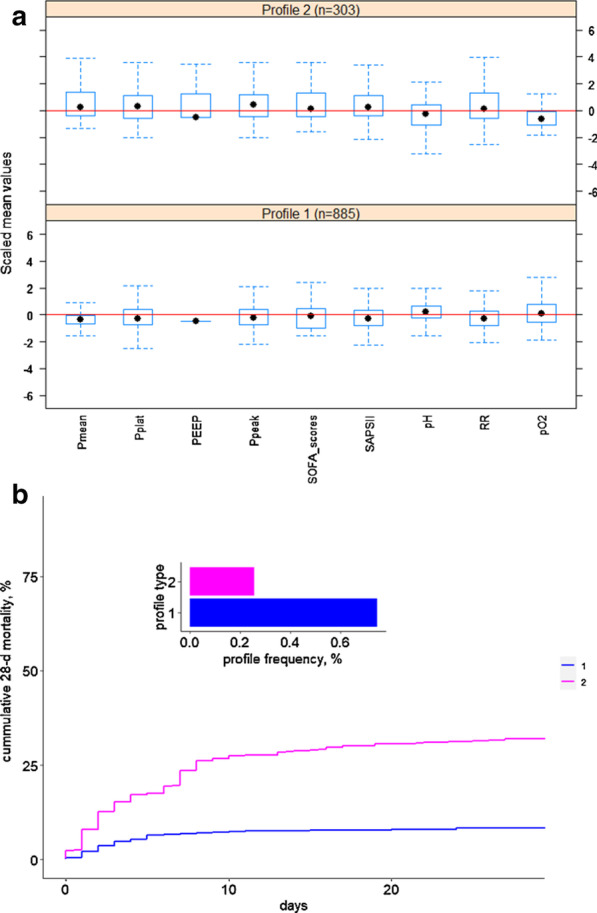
Based on 36 characteristic variables, we divided patients undergoing mechanical ventilation and sedation and analgesia into two categories with different mortality rates, then further reduced the dimensionality of the data and obtained the 9 variables that had the greatest impact on classification, most of which were ventilator parameters. According to the Richmond-ASS scores, the two phenotypes of patients had different degrees of sedation and analgesia, and the corresponding ventilator parameters were also significantly different. We divided the validation cohort into three different levels of sedation, revealing that patients with high ventilator conditions needed a deeper level of sedation, while patients with low ventilator conditions required reduction in the depth of sedation as soon as possible to promote recovery and avoid reinjury.
Through latent profile analysis and dimensionality reduction, we divided patients treated with mechanical ventilation and sedation and analgesia into two categories with different mortalities and obtained 9 variables that had the greatest impact on classification, which revealed that the depth of sedation was limited by the condition of the respiratory system.
镇痛镇静治疗在危重症患者中,尤其是机械通气患者中被广泛应用。镇痛镇静治疗的理解从最初的非镇静方案到深度镇静,再到按需镇静,不断深入。然而,根据不同患者的病情,对于个体患者的镇静深度需求仍不明确。
本研究使用了公开的危重患者数据库 Medical Information Mart for Intensive Care III。采用潜在剖面分析作为聚类方法,根据 36 个变量对机械通气患者进行分类。采用主成分分析降维方法选择最有影响的变量。使用 ROC 曲线评估模型的分类准确性。
基于 36 个特征变量,我们将接受机械通气和镇静镇痛的患者分为死亡率不同的两类,然后进一步降低数据的维度,得到对分类影响最大的 9 个变量,其中大部分是呼吸机参数。根据 Richmond-ASS 评分,这两种患者表型的镇静镇痛程度不同,相应的呼吸机参数也有显著差异。我们将验证队列分为三个不同的镇静水平,揭示出高呼吸机条件的患者需要更深层次的镇静,而低呼吸机条件的患者需要尽快降低镇静深度,以促进恢复并避免再次损伤。
通过潜在剖面分析和降维,我们将接受机械通气和镇静镇痛治疗的患者分为死亡率不同的两类,并获得了对分类影响最大的 9 个变量,结果表明镇静深度受到呼吸系统状况的限制。