Department of Imaging Physics, The University of Texas MD Anderson Cancer Center, Houston, Texas, USA.
The University of Texas Graduate School of Biomedical Sciences at Houston, Houston, Texas, USA.
Med Phys. 2021 Oct;48(10):6226-6236. doi: 10.1002/mp.15147. Epub 2021 Aug 18.
Colorectal cancer is the third most common form of cancer in the United States, and up to 60% of these patients develop liver metastasis. While hepatic resection is the curative treatment of choice, only 20% of patients are candidates at the time of diagnosis. While percutaneous thermal ablation (PTA) has demonstrated 24%-51% overall 5-year survival rates, assurance of sufficient ablation margin delivery (5 mm) can be challenging, with current methods of 2D distance measurement not ensuring 3D minimum margin. We hypothesized that biomechanical model-based deformable image registration (DIR) can reduce spatial uncertainties and differentiate local tumor progression (LTP) patients from LTP-free patients.
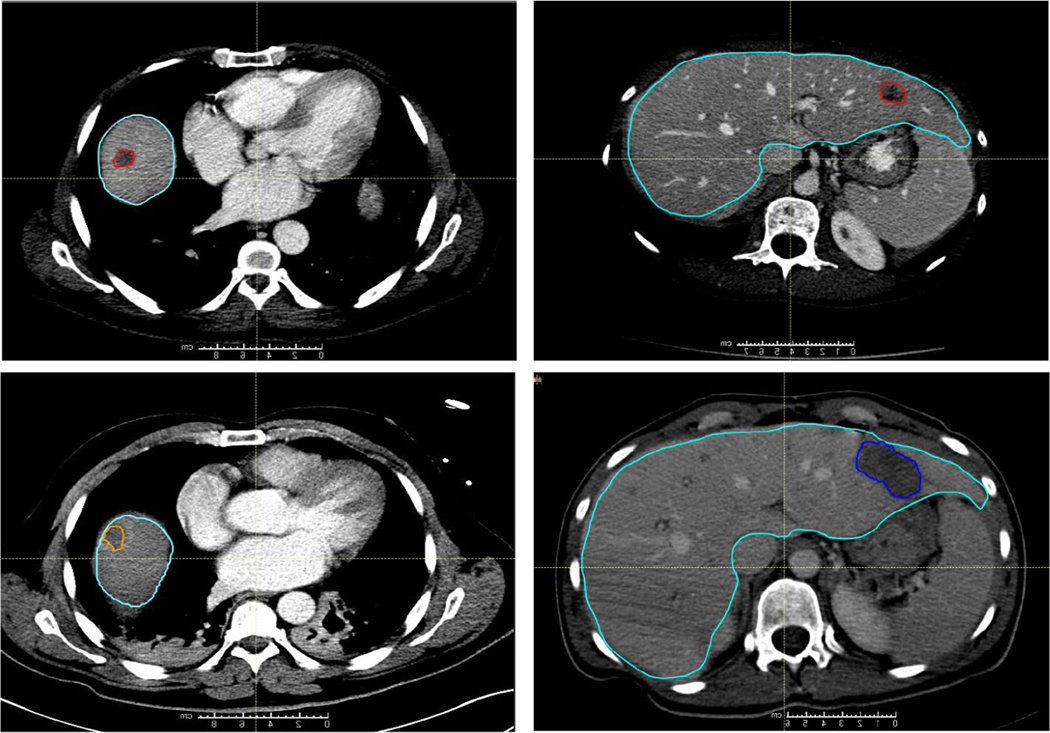
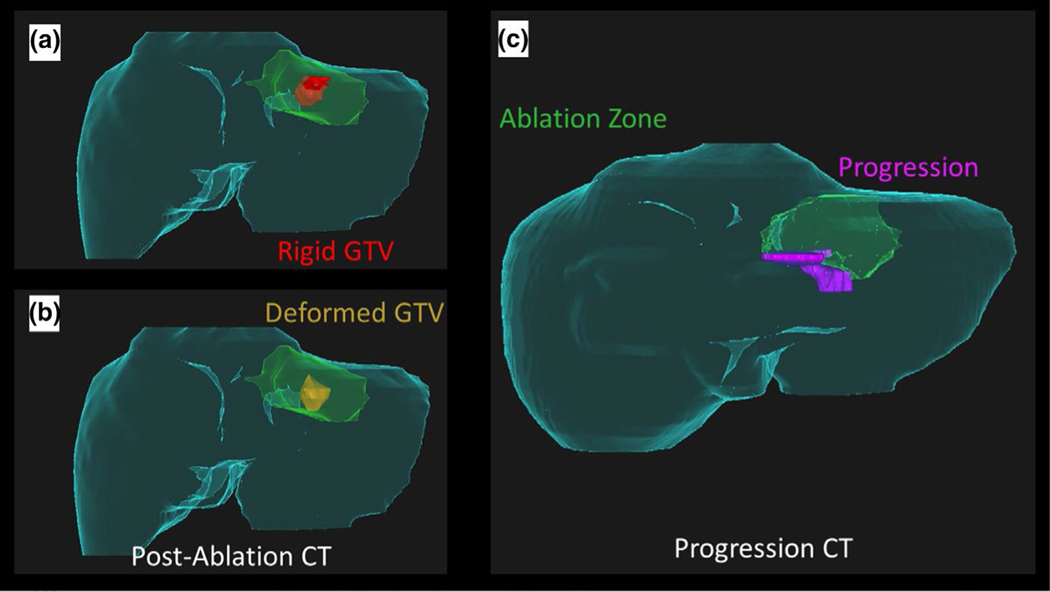
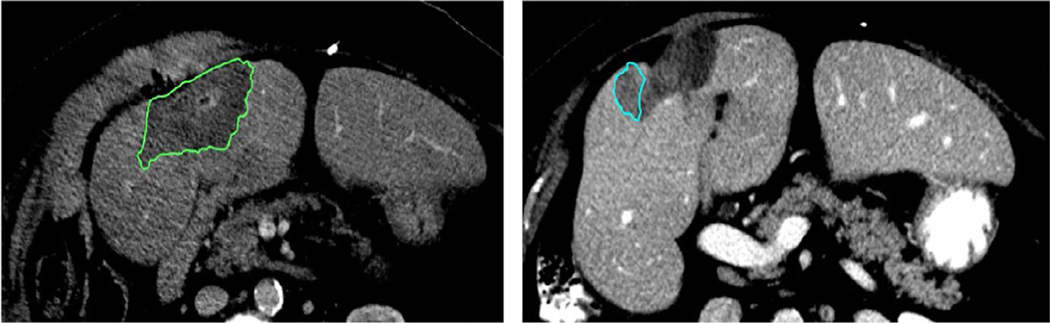
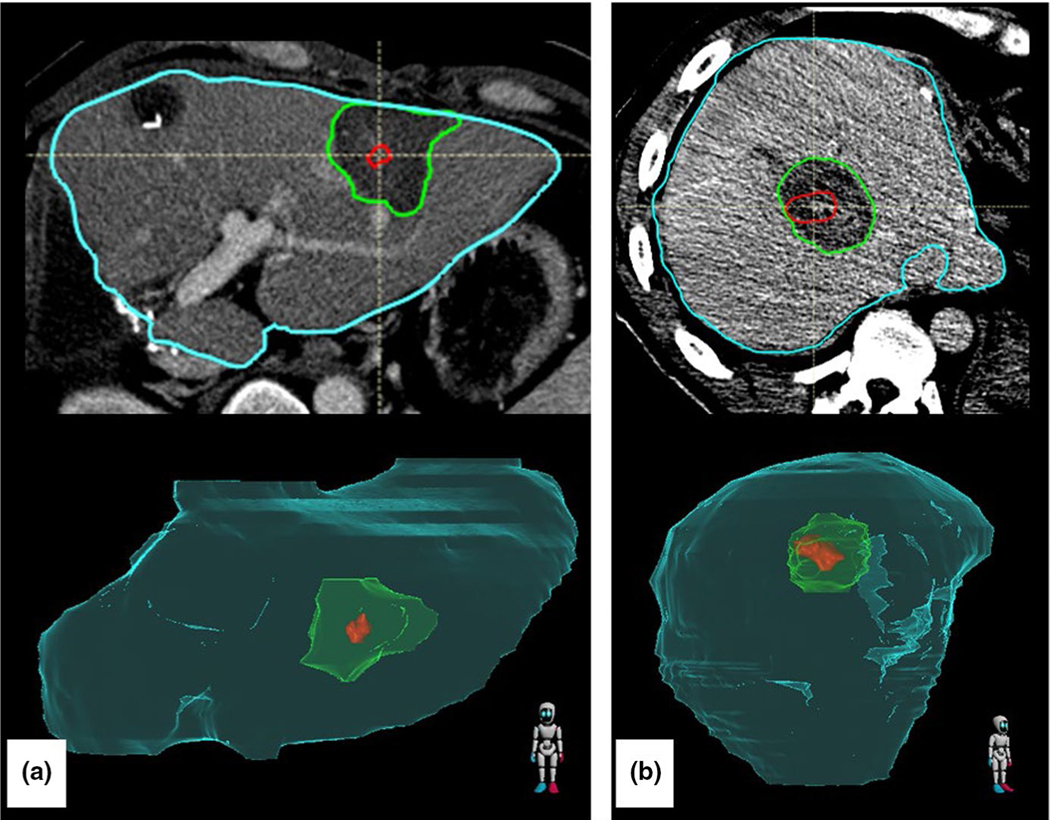
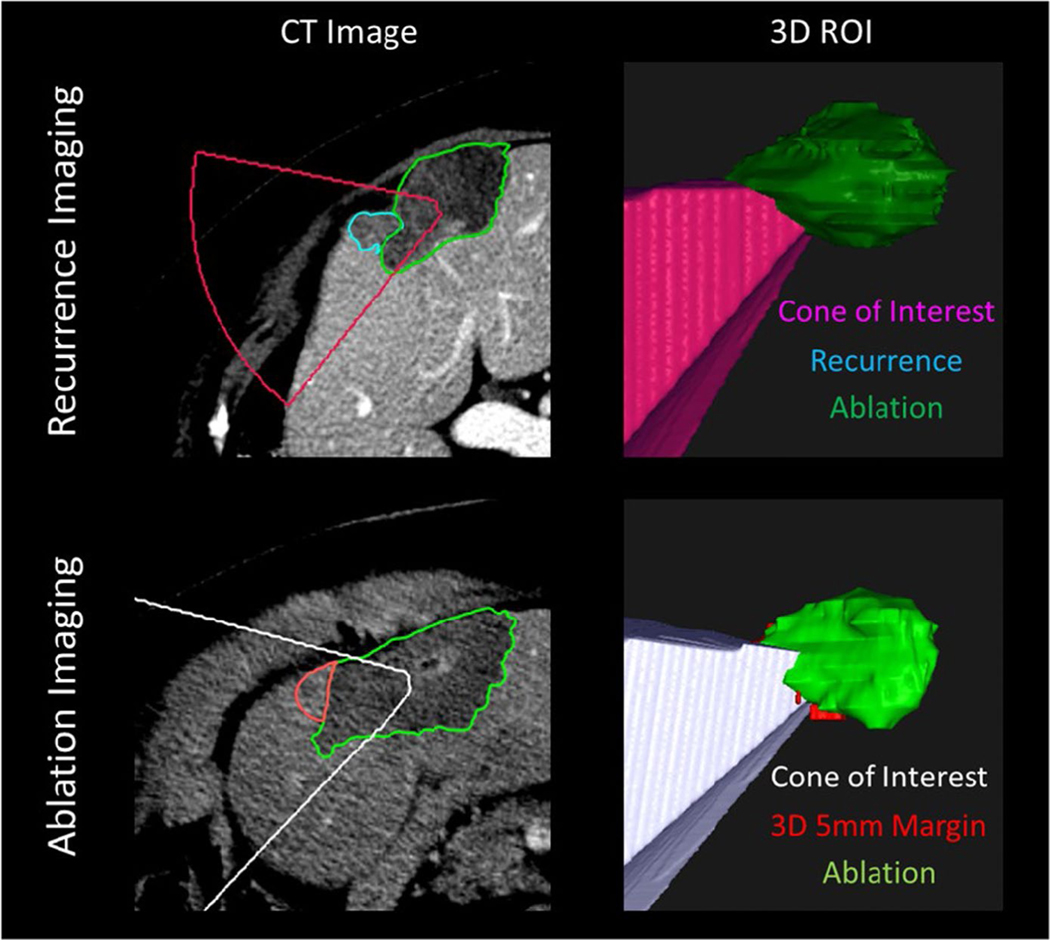
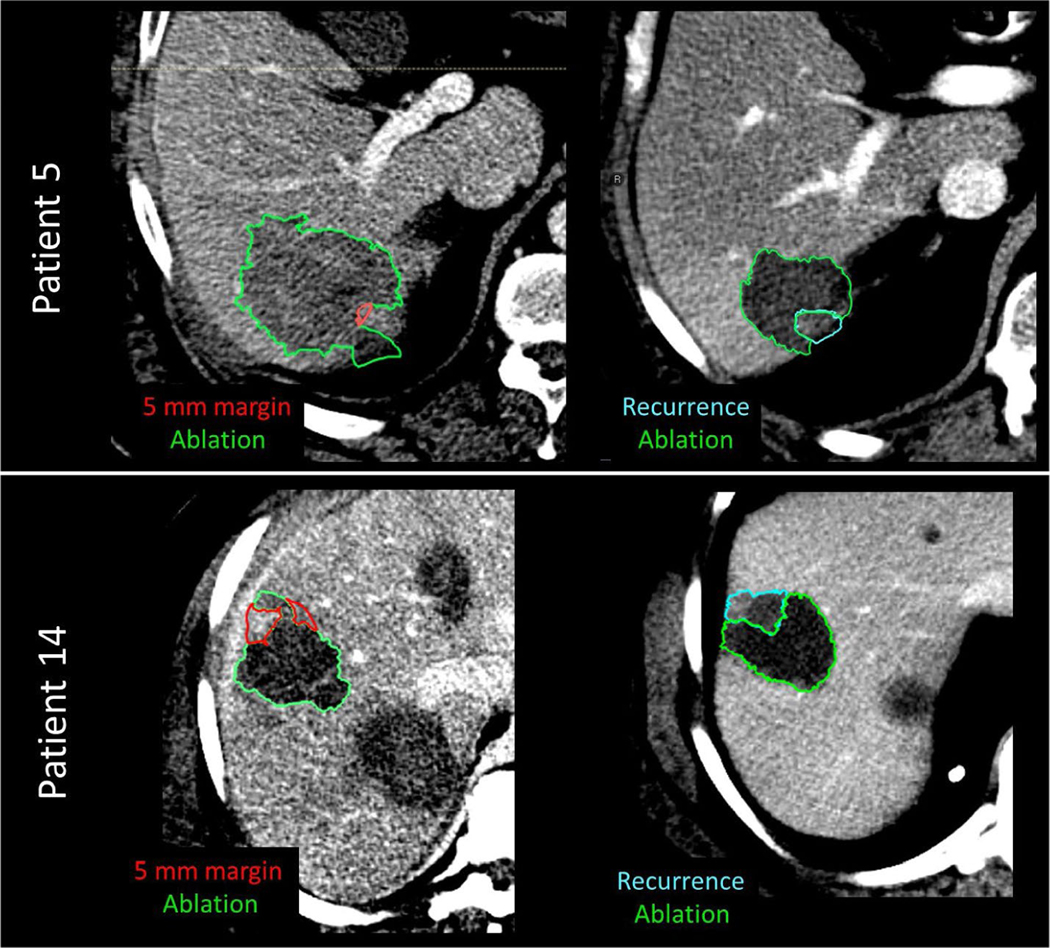
We retrospectively acquired 30 patients (16 LTP and 14 LTP-free) at our institution who had undergone PTA and had a contrast-enhanced pre-treatment and post-ablation CT scan. Liver, disease, and ablation zone were manually segmented. Biomechanical model-based DIR between the pre-treatment and post-ablation CT mapped the gross tumor volume onto the ablation zone and measured 3D minimum delivered margin (MDM). An in-house cone-tracing algorithm determined if progression qualitatively collocated with insufficient 5 mm margin achieved.
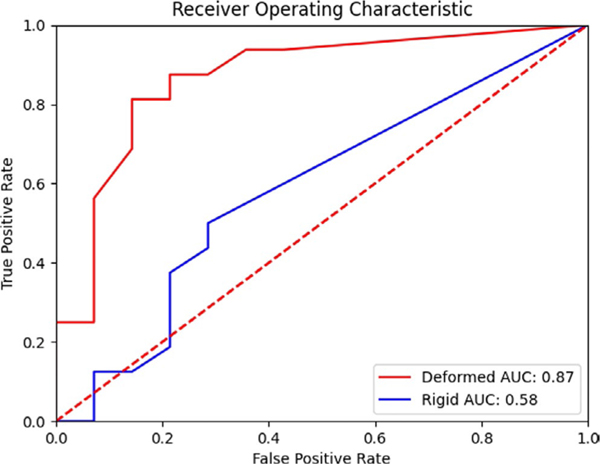
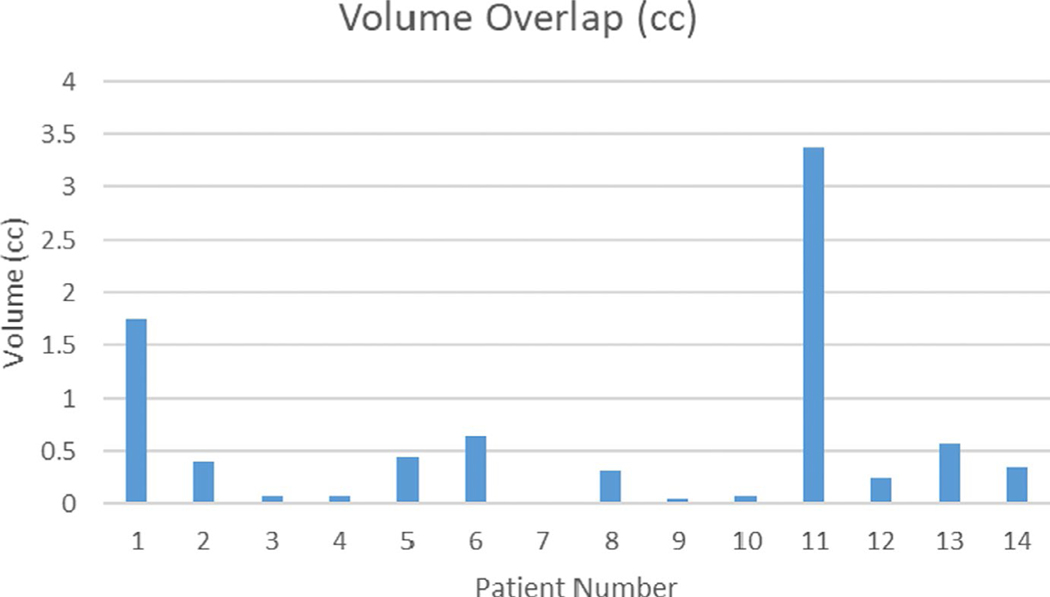
Mann-Whitney U test showed a significant difference (p < 0.01) in MDM from the LTP and LTP-free groups. A total of 93% (13/14) of patients with LTP had a correlation between progression and missing 5 mm of margin volume.
Biomechanical DIR is able to reduce spatial uncertainty and allow measurement of delivered 3D MDM. This minimum margin can help ensure sufficient ablation delivery, and our workflow can provide valuable information in a clinically useful timeframe.
结直肠癌是美国第三大常见癌症类型,多达 60%的患者会发展为肝转移。虽然肝切除术是治疗的首选方法,但只有 20%的患者在诊断时符合手术条件。虽然经皮热消融(PTA)的总 5 年生存率为 24%-51%,但保证足够的消融边界(5 毫米)可能具有挑战性,目前的二维距离测量方法并不能确保 3D 最小边界。我们假设基于生物力学模型的变形图像配准(DIR)可以减少空间不确定性,并区分局部肿瘤进展(LTP)患者和无 LTP 患者。
我们回顾性地从本机构获得了 30 名患者(16 名 LTP 和 14 名无 LTP),这些患者接受了 PTA 治疗,并进行了增强的术前和术后 CT 扫描。手动分割肝脏、病变和消融区。基于生物力学模型的 DIR 将术前和术后 CT 中的大体肿瘤体积映射到消融区,并测量 3D 最小递送边界(MDM)。内部锥体追踪算法确定进展是否定性上与未达到 5 毫米的最小边界一致。
Mann-Whitney U 检验显示,LTP 和无 LTP 组的 MDM 存在显著差异(p<0.01)。14 名无 LTP 患者中,有 93%(13/14)的患者在进展与缺少 5 毫米边界体积之间存在相关性。
生物力学 DIR 能够减少空间不确定性并允许测量递送的 3D MDM。这个最小边界可以帮助确保足够的消融输送,我们的工作流程可以在临床有用的时间内提供有价值的信息。