Medical Research Council Biostatistics Unit, School of Clinical Medicine, University of Cambridge, Cambridge, UK.
UK Health Security Agency, London, UK.
Nat Commun. 2022 Aug 17;13(1):4834. doi: 10.1038/s41467-022-32458-y.
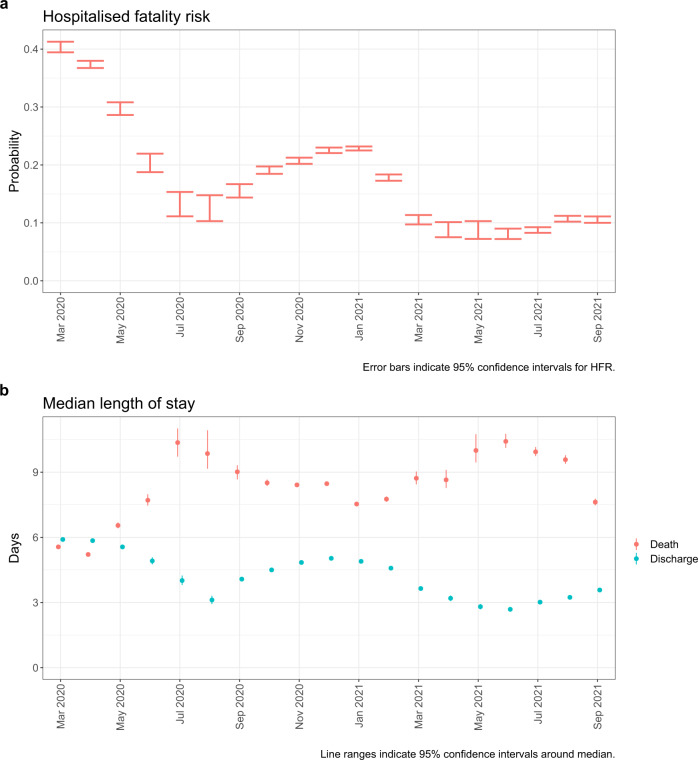
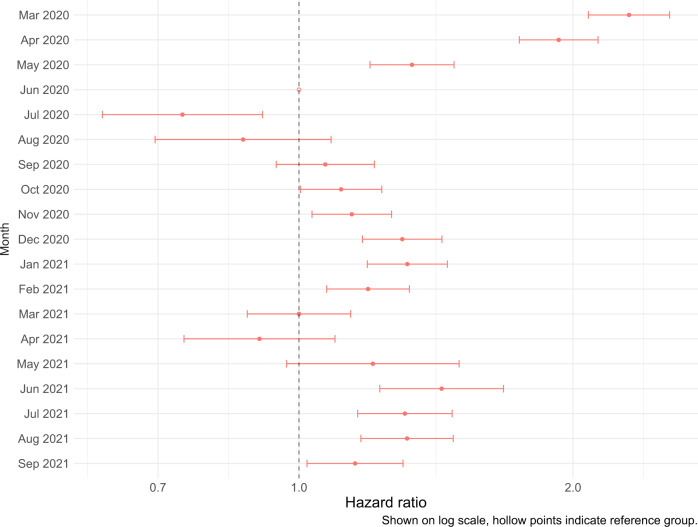
Widespread vaccination campaigns have changed the landscape for COVID-19, vastly altering symptoms and reducing morbidity and mortality. We estimate trends in mortality by month of admission and vaccination status among those hospitalised with COVID-19 in England between March 2020 to September 2021, controlling for demographic factors and hospital load. Among 259,727 hospitalised COVID-19 cases, 51,948 (20.0%) experienced mortality in hospital. Hospitalised fatality risk ranged from 40.3% (95% confidence interval 39.4-41.3%) in March 2020 to 8.1% (7.2-9.0%) in June 2021. Older individuals and those with multiple co-morbidities were more likely to die or else experienced longer stays prior to discharge. Compared to unvaccinated people, the hazard of hospitalised mortality was 0.71 (0.67-0.77) with a first vaccine dose, and 0.56 (0.52-0.61) with a second vaccine dose. Compared to hospital load at 0-20% of the busiest week, the hazard of hospitalised mortality during periods of peak load (90-100%), was 1.23 (1.12-1.34). The prognosis for people hospitalised with COVID-19 in England has varied substantially throughout the pandemic and according to case-mix, vaccination, and hospital load. Our estimates provide an indication for demands on hospital resources, and the relationship between hospital burden and outcomes.
广泛的疫苗接种运动改变了 COVID-19 的局面,极大地改变了症状,并降低了发病率和死亡率。我们估计了 2020 年 3 月至 2021 年 9 月期间在英格兰因 COVID-19 住院的患者中按入院月份和疫苗接种状况划分的死亡率趋势,同时控制了人口统计学因素和医院负担。在 259727 例因 COVID-19 住院的患者中,有 51948 例(20.0%)在住院期间死亡。住院病死率从 2020 年 3 月的 40.3%(95%置信区间 39.4-41.3%)降至 2021 年 6 月的 8.1%(7.2-9.0%)。年龄较大的患者和患有多种合并症的患者更有可能死亡,或在出院前经历更长的住院时间。与未接种疫苗的人相比,首次接种疫苗的住院死亡风险为 0.71(0.67-0.77),第二次接种疫苗的风险为 0.56(0.52-0.61)。与医院负荷处于最繁忙周的 0-20%相比,在高峰期(90-100%)的住院死亡风险为 1.23(1.12-1.34)。英格兰 COVID-19 住院患者的预后在整个大流行期间以及根据病例组合、疫苗接种和医院负荷而有了显著变化。我们的估计为医院资源需求提供了一个指标,并说明了医院负担与结局之间的关系。