From the Population Health Research Institute (A.S., M.O.D., S.R., S.Y.), McMaster University and Hamilton Health Sciences, ON, Canada; HRB Clinical Research Facility Galway (A.S., M.O.D., M.C., C.M.), Department of Medicine, University of Galway, Ireland; Medical School (G.J.H.), Faculty of Health and Medical Sciences, The University of Western Australia, Perth, Australia; Rush Alzheimer Disease Research Center (S.O.), Rush University Medical Center, Chicago, IL; St John's Medical College and Research Institute (D.X.), Bangalore, India; Beijing Hypertension League Institute (H.Z.), China; Faculty of Medicine (A.D.), Eduardo Mondlane University, Maputo, Mozambique; Hospital Alemao Oswaldo Cruz (A.A.), Sao Paulo, Brazil; National Medical Research Center of Cardiology (N.P.), Moscow, Russia; Department of Internal Medicine (A.O.), Faculty of Medicine, Istanbul Medeniyet University, Turkey; Military Institute of Aviation Medicine (D.R.), Warsaw, Poland; Stroke Center (H.K.I.), Department of Neurology, Rigshospitalet, University of Copenhagen, Denmark; Faculty of Medicine (F.L.), Universidad de La Frontera, Temuco, Chile; Sahlgrenska University Hospital and Sahlgrenska Academy (A.R.), University of Gothenburg, Sweden; and Academic Section of Geriatric Medicine (P.L.), Glasgow Royal Infirmary, University of Glasgow, United Kingdom.
Neurology. 2023 Jan 10;100(2):e142-e153. doi: 10.1212/WNL.0000000000201388. Epub 2022 Oct 11.
There is uncertainty about the association between alcohol consumption and stroke, particularly for low-moderate intake. We explored these associations in a large international study.
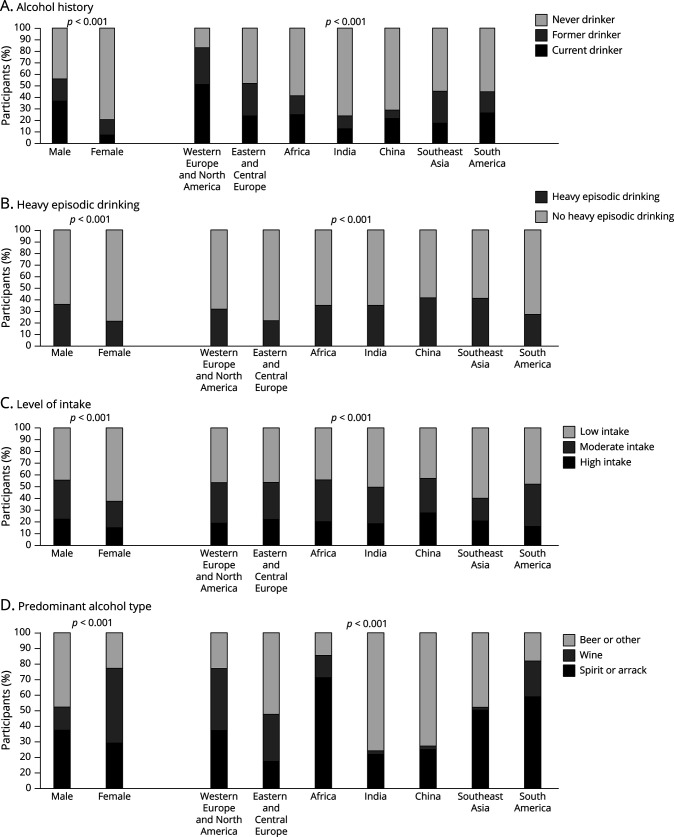
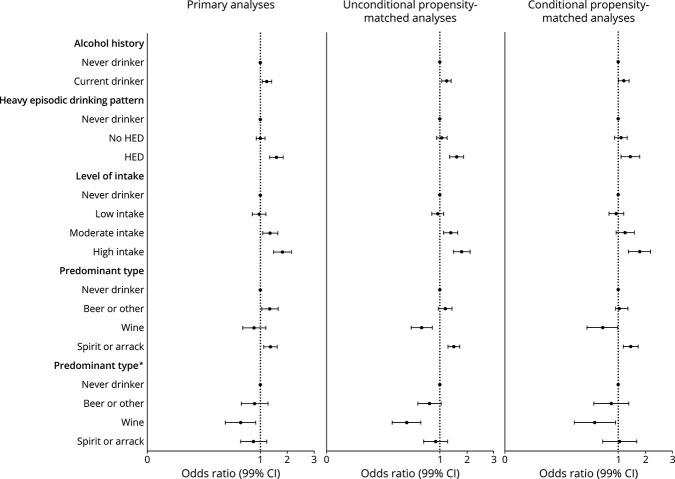
INTERSTROKE, a case-control study, is the largest international study of risk factors for acute stroke. Alcohol consumption was self-reported and categorized by drinks/week as low (1-7), moderate (7-14 for females and 7-21 for males), or high (>14 for females and >21 for males). Heavy episodic drinking (HED) was defined as >5 drinks on ≥1 day per month. Multivariable conditional logistic regression was used to determine associations.
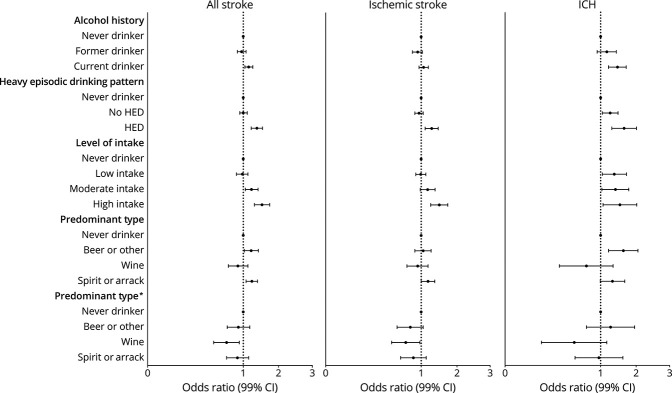
We included 12,913 cases and 12,935 controls; 25.0% (n = 6,449) were current drinkers, 16.7% (n = 4,318) former drinkers, and 58.3% (n = 15,076) never drinkers. Current drinkers were younger, male, smokers, active, and with higher-paid occupations. Current drinking was associated with all stroke (OR 1.14; 95% CI 1.04-1.26) and intracerebral hemorrhage (ICH) (OR 1.50, 95% CI 1.21-1.84) but not ischemic stroke (OR 1.06; 95% CI 0.95-1.19). HED pattern was associated with all stroke (OR 1.39; 95% CI 1.21-1.59), ischemic stroke (OR 1.29; 95% CI 1.10-1.51), and ICH (OR 1.76; 95% CI 1.31-2.36). High level of alcohol intake was consistently associated with all stroke, ischemic stroke, and ICH. Moderate intake was associated with all stroke and ICH but not ischemic stroke. Low alcohol intake was not associated with stroke overall, but there were regional differences; low intake was associated with reduced odds of stroke in Western Europe/North America (OR 0.66; 95% CI 0.45-0.96) and increased odds in India (OR 2.18; 95% CI 1.42-3.36) (p-interaction 0.037). Wine consumption was associated with reduced odds of all stroke and ischemic stroke but not ICH. The magnitudes of association were greatest in those without hypertension and current smokers.
High and moderate intake were associated with increased odds of stroke, whereas low intake was not associated with stroke. However, there were important regional variations, which may relate to differences in population characteristics of alcohol consumers, types or patterns of consumption.
关于饮酒与中风之间的关联存在不确定性,尤其是对于低-中度饮酒者。我们在一项大型国际研究中对这些关联进行了探索。
INTERSTROKE 是一项病例对照研究,是针对急性中风危险因素的最大型国际研究。饮酒情况由自我报告,每周饮酒量(单位:杯)分类为低(女性 1-7 杯,男性 7-21 杯)、中(女性 7-14 杯,男性 7-21 杯)或高(女性 >14 杯,男性 >21 杯)。重度间歇性饮酒(HED)定义为每月≥1 天内饮用>5 杯酒。采用多变量条件逻辑回归确定关联。
我们纳入了 12913 例病例和 12935 例对照;25.0%(n=6449)为当前饮酒者,16.7%(n=4318)为既往饮酒者,58.3%(n=15076)为从不饮酒者。当前饮酒者更年轻、男性、吸烟者、活跃、从事高薪职业。当前饮酒与所有中风(OR 1.14;95%CI 1.04-1.26)和脑内出血(ICH)(OR 1.50,95%CI 1.21-1.84)相关,但与缺血性中风(OR 1.06;95%CI 0.95-1.19)无关。HED 模式与所有中风(OR 1.39;95%CI 1.21-1.59)、缺血性中风(OR 1.29;95%CI 1.10-1.51)和 ICH(OR 1.76;95%CI 1.31-2.36)均相关。高饮酒量始终与所有中风、缺血性中风和 ICH 相关。中等饮酒量与所有中风和 ICH 相关,但与缺血性中风无关。低饮酒量与总体中风无关,但存在地域差异;在西欧/北美,低饮酒量与中风风险降低相关(OR 0.66;95%CI 0.45-0.96),在印度,与中风风险升高相关(OR 2.18;95%CI 1.42-3.36)(p 交互作用=0.037)。葡萄酒消费与所有中风和缺血性中风风险降低相关,但与 ICH 无关。在没有高血压和当前吸烟者中,关联的程度最大。
高和中量饮酒与中风风险增加相关,而低量饮酒与中风无关。然而,存在重要的地域差异,这可能与饮酒人群的人口特征、消费类型或模式的差异有关。