Warwick Medical School, University of Warwick, Coventry, UK.
Centre for Sport, Exercise and Life Sciences, Faculty of Health and Life Sciences, Coventry University, Coventry, UK.
ESC Heart Fail. 2023 Aug;10(4):2487-2498. doi: 10.1002/ehf2.14422. Epub 2023 Jun 6.
Comorbidities play a significant role towards the pathophysiology of heart failure with preserved ejection fraction (HFpEF), characterized by abnormal macrovascular function and altered ventricular-vascular coupling. However, our understanding of the role of comorbidities and arterial stiffness in HFpEF remains incomplete. We hypothesized that HFpEF is preceded by a cumulative rise in arterial stiffness as cardiovascular comorbidities accumulate, beyond that associated with ageing.
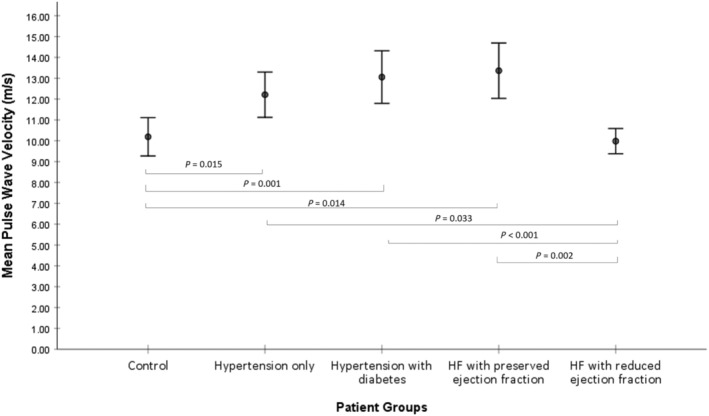
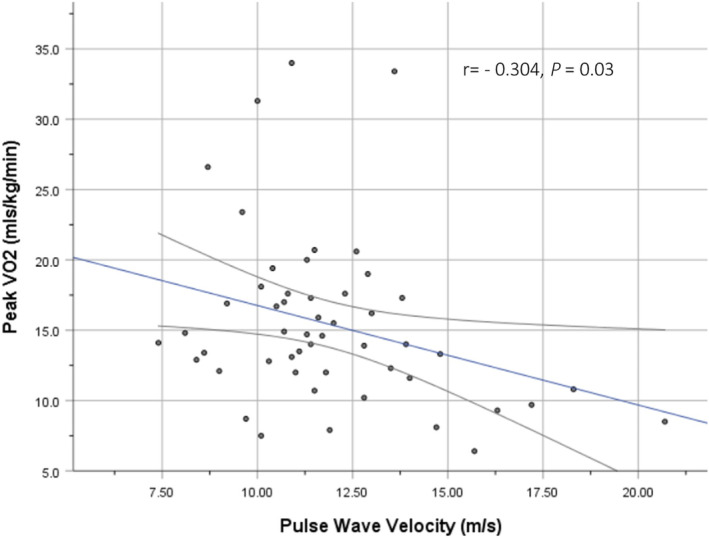
Arterial stiffness was assessed using pulse wave velocity (PWV) in five groups: Group A, healthy volunteers (n = 21); Group B, patients with hypertension (n = 21); Group C, hypertension and diabetes mellitus (n = 20); Group D, HFpEF (n = 21); and Group E, HF with reduced ejection fraction (HFrEF) (n = 11). All patients were aged 70 and above. Mean PWV increased from Groups A to D (PWV 10.2, 12.2, 13.0, and 13.7 m/s, respectively) as vascular comorbidities accumulated independent of age, renal function, haemoglobin, obesity (body mass index), smoking status, and hypercholesterolaemia. HFpEF exhibited the highest PWV and HFrEF displayed near-normal levels (13.7 vs. 10 m/s, P = 0.003). PWV was inversely related to peak oxygen consumption (r = -0.304, P = 0.03) and positively correlated with left ventricular filling pressures (E/e') on echocardiography (r = -0.307, P = 0.014).
This study adds further support to the concept of HFpEF as a disease of the vasculature, underlined by an increasing arterial stiffness that is driven by vascular ageing and accumulating vascular comorbidities, for example, hypertension and diabetes. Reflecting a pulsatile arterial afterload associated with diastolic dysfunction and exercise capacity, PWV may provide a clinically relevant tool to identify at-risk intermediate phenotypes (e.g. pre-HFpEF) before overt HFpEF occurs.
合并症在射血分数保留型心力衰竭(HFpEF)的病理生理学中起着重要作用,其特征为大血管功能异常和心室血管耦联改变。然而,我们对合并症和动脉僵硬度在 HFpEF 中的作用的理解仍不完整。我们假设,HFpEF 是在心血管合并症累积导致动脉僵硬度逐渐升高的情况下发生的,这种升高超出了与年龄相关的升高。
使用脉搏波速度(PWV)评估动脉僵硬度,分为五组:A 组,健康志愿者(n=21);B 组,高血压患者(n=21);C 组,高血压合并糖尿病患者(n=20);D 组,HFpEF 患者(n=21);E 组,射血分数降低的心力衰竭(HFrEF)患者(n=11)。所有患者年龄均在 70 岁以上。随着血管合并症的累积,PWV 从 A 组到 D 组逐渐升高(PWV 分别为 10.2、12.2、13.0 和 13.7m/s),与年龄、肾功能、血红蛋白、肥胖(体重指数)、吸烟状况和高胆固醇血症无关。HFpEF 组的 PWV 最高,HFrEF 组的 PWV 接近正常水平(13.7 与 10m/s,P=0.003)。PWV 与峰值耗氧量呈负相关(r=-0.304,P=0.03),与超声心动图上的左心室充盈压(E/e')呈正相关(r=-0.307,P=0.014)。
本研究进一步支持 HFpEF 是一种血管疾病的概念,其特征是动脉僵硬度逐渐升高,这种升高是由血管老化和血管合并症(如高血压和糖尿病)引起的。PWV 反映了与舒张功能障碍和运动能力相关的脉动性动脉后负荷,可能为识别明显 HFpEF 之前的高危中间表型(例如,HFpEF 前)提供一种有临床意义的工具。