Deshmukh Shobit, Gupta Nirav, Heo Ki Seong, Shon Won Yong, Jo Se Myoung, Pancholiya Anshul
Department of Orthopaedic Surgery, Busan Bumin Hospital, Busan, Korea.
Hip Pelvis. 2024 Sep 1;36(3):187-195. doi: 10.5371/hp.2024.36.3.187.
Pelvis tilting in sagittal plane influences the acetabular cup position. Majority of total hip arthroplasty (THA) are performed in lateral decubitus surgical position. This study is to assess whether there is any difference in sacral slope between standing and lateral decubitus position and influence of this variation in planning acetabular cup anteversion.
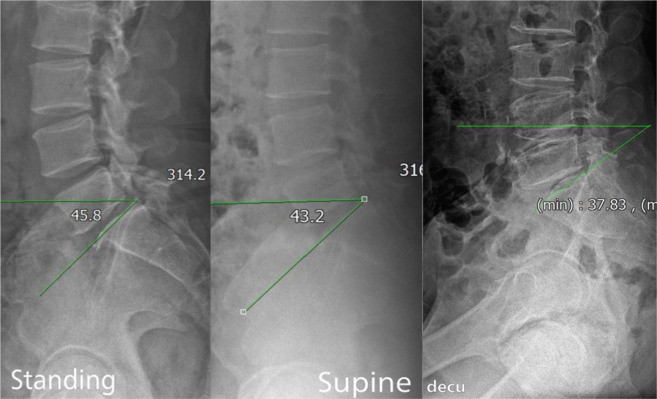
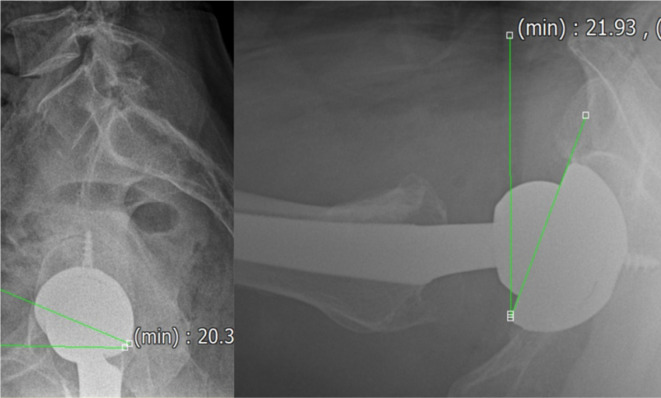
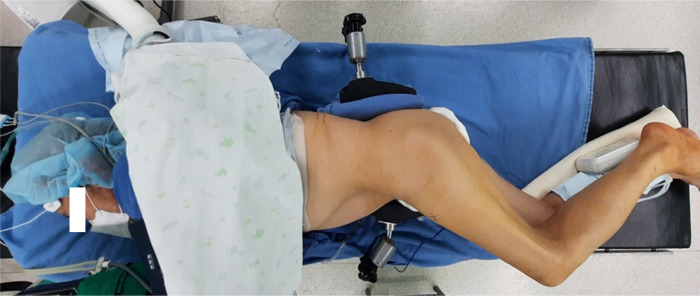
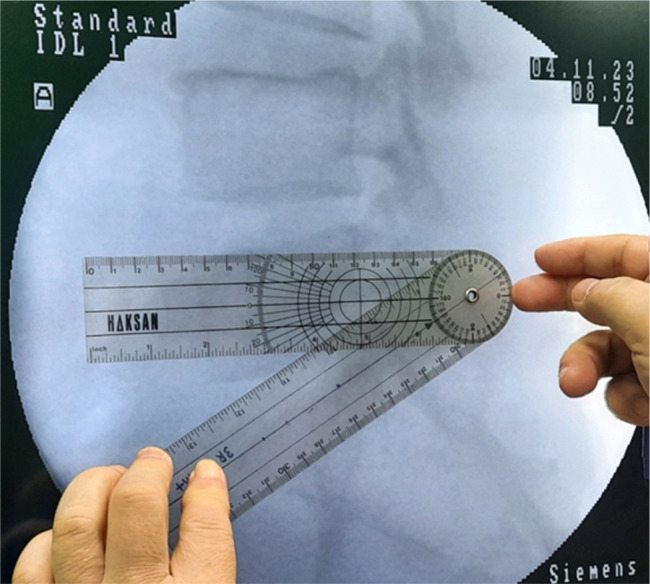
This is a prospective study including 50 patients operated between January 2020 to March 2022. Preoperative radiograph included lumbosacral spine lateral X-ray in standing, supine and lateral decubitus positions to calculate the sacral slope for assessment of anterior or posterior pelvic tilting. In our study, we determined the position of the acetabular cup based on changes in sacral slope between standing and lateral decubitus postures. For patients whose sacral slope increased from lateral decubitus to standing, we implanted the acetabular component with a higher degree of anteversion. Conversely, for patients with reverse phenomenon, the cup was inserted at lower anteversion.
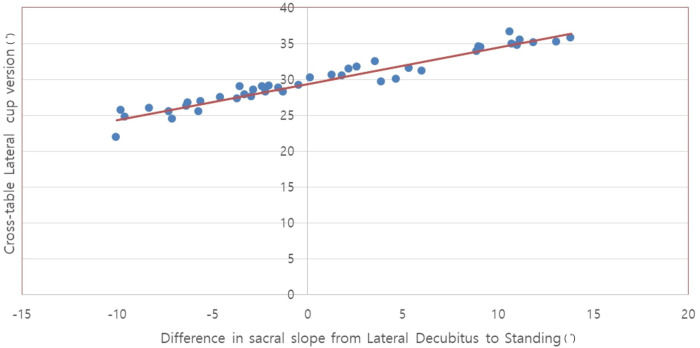
Twenty-four patients (48.0%) had increase in sacral slope from lateral decubitus to standing whereas 26 patients (52.0%) had decrease in sacral slope. There was linear correlation between difference in preoperative sacral slope and postoperative cross table lateral cup anteversion. Harris hip scores improved from 40.78 to 85.43. There was no subluxation or dislocation in any patient at minimum 2-year follow-up.
Individualized acetabular cup placement is important for better functional outcome in THA. Evaluation of pelvic tilting in lateral decubitus position is necessary for better positioning of acetabular cup and avoid postoperative complications.
骨盆在矢状面的倾斜会影响髋臼杯的位置。大多数全髋关节置换术(THA)是在侧卧位手术体位下进行的。本研究旨在评估站立位和侧卧位时骶骨斜率是否存在差异,以及这种变化对髋臼杯前倾角规划的影响。
这是一项前瞻性研究,纳入了2020年1月至2022年3月间接受手术的50例患者。术前影像学检查包括站立位、仰卧位和侧卧位的腰骶部脊柱侧位X线片,以计算骶骨斜率,评估骨盆前倾或后倾。在我们的研究中,我们根据站立位和侧卧位之间骶骨斜率的变化来确定髋臼杯的位置。对于骶骨斜率从侧卧位到站立位增加的患者,我们植入前倾角度更大的髋臼组件。相反,对于出现相反现象的患者,髋臼杯以前倾角度较小的方式植入。
24例患者(48.0%)骶骨斜率从侧卧位到站立位增加,而26例患者(52.0%)骶骨斜率降低。术前骶骨斜率差异与术后髋臼杯交叉台侧位前倾角之间存在线性相关性。Harris髋关节评分从40.78提高到85.43。在至少2年的随访中,没有患者出现半脱位或脱位。
个体化的髋臼杯放置对于THA获得更好的功能结果很重要。评估侧卧位时的骨盆倾斜对于更好地定位髋臼杯和避免术后并发症是必要的。