Gaïni Shahin, Pedersen Svend Stenvang, Koldkjaer Ole Graesbøll, Pedersen Court, Møller Holger Jon
Department of Infectious Diseases, Odense University Hospital, Søndre Boulevard 29, DK-5000 Odense C, Denmark.
Crit Care. 2007;11(2):R32. doi: 10.1186/cc5715.
Sepsis is a serious condition with a significant morbidity and mortality. New insight into the immunopathogenesis of sepsis could promote the development of new strategies for diagnosis and therapy. High mobility group box-1 protein (HMGB1) has been known for many years as a nuclear chromosomal protein. Its role as a pro-inflammatory cytokine in sepsis and rheumatoid arthritis has been described recently. The aim of our study was to evaluate HMGB1 as a molecular marker in patients with community-acquired infections.
Patients suspected of having infections/sepsis and admitted to a department of internal medicine were included in the study in a prospective manner. Demographic data, comorbidity, routine biochemistry, microbiological data, infection focus, severity score, and mortality on day 28 were recorded. Plasma and serum were sampled at the time of admission. HMGB1 levels were measured with a commercially available enzyme-linked immunosorbent assay (ELISA). Procalcitonin levels were measured with a TRACE (time-resolved amplified cryptate emission) assay. Lipopolysaccharide-binding protein and interleukin-6 were measured with a chemiluminiscent immunometric assay. Soluble haemoglobin scavenger receptor (sCD163) levels were measured with an in-house ELISA.
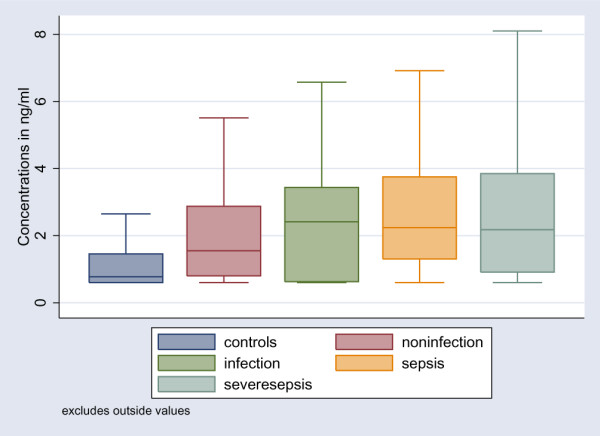
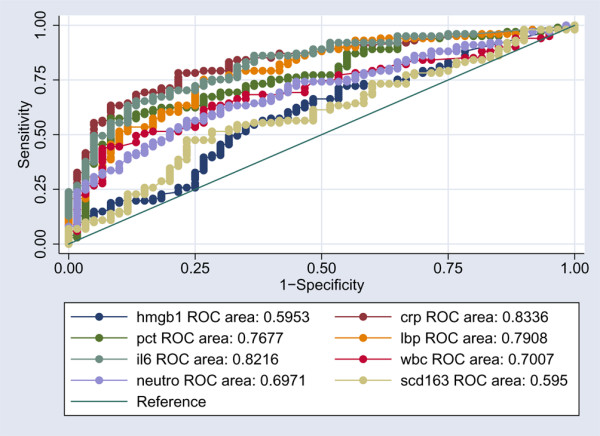
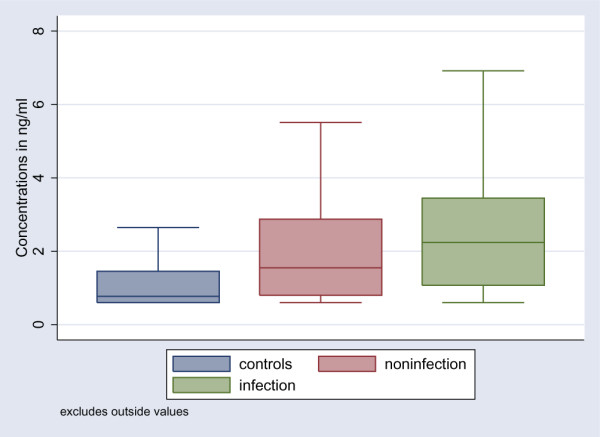
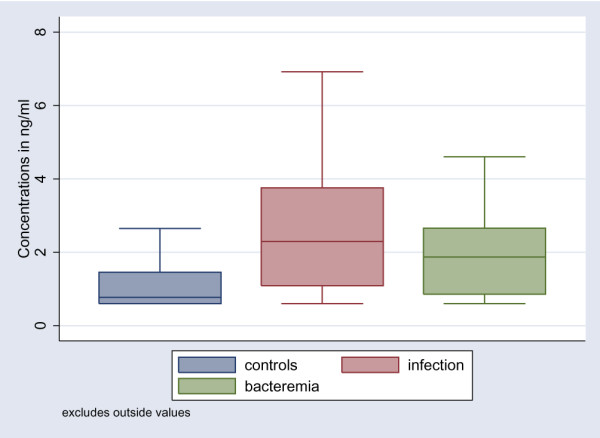
One hundred and ninety-four patients were included in the study. Levels of HMGB1 are presented as medians and interquartile ranges: healthy controls (0.77 ng/ml, 0.6 to 1.46), non-infected patients (1.54 ng/ml, 0.79 to 2.88), infected patients without systemic inflammatory response syndrome (2.41 ng/ml, 0.63 to 3.44), patients with sepsis (2.24 ng/ml, 1.30 to 3.75), and patients with severe sepsis (2.18 ng/ml, 0.91 to 3.85). In a receiver operator characteristic curve analysis discriminating between non-infected patients and all infected patients, the area under the curve for HMGB1 was 0.59 (P < 0.0001). HMGB1 correlated only weakly to levels of white blood cell count, neutrophils, C-reactive protein, interleukin-6, procalcitonin, and lipopolysaccharide-binding protein (P < 0.001). HMGB1 did not correlate to sCD163.
In a cohort of patients with suspected community-acquired infections and sepsis, HMGB1 levels were statistically significantly higher in patients compared to the healthy controls. There was no statistically significant difference between the infected and the non-infected patients. Levels of HMGB1 correlated only very weakly to other pro-inflammatory markers and did not correlate to the anti-inflammatory marker sCD163.
脓毒症是一种严重的病症,具有较高的发病率和死亡率。对脓毒症免疫发病机制的新认识可能会促进诊断和治疗新策略的发展。高迁移率族蛋白B1(HMGB1)多年来一直被认为是一种核染色体蛋白。其作为脓毒症和类风湿性关节炎中促炎细胞因子的作用最近已有描述。我们研究的目的是评估HMGB1作为社区获得性感染患者的分子标志物。
前瞻性纳入怀疑有感染/脓毒症并入住内科的患者。记录人口统计学数据、合并症、常规生化指标、微生物学数据、感染灶、严重程度评分及28天死亡率。入院时采集血浆和血清。采用市售酶联免疫吸附测定(ELISA)法检测HMGB1水平。采用时间分辨荧光免疫分析(TRACE)法检测降钙素原水平。采用化学发光免疫分析法检测脂多糖结合蛋白和白细胞介素-6。采用自制ELISA法检测可溶性血红蛋白清除受体(sCD163)水平。
194例患者纳入研究。HMGB1水平以中位数和四分位数间距表示:健康对照者(0.77 ng/ml,0.6至1.46)、未感染患者(1.54 ng/ml,0.79至2.88)、无全身炎症反应综合征的感染患者(2.41 ng/ml,0.63至3.44)、脓毒症患者(2.24 ng/ml,1.30至3.75)和严重脓毒症患者(2.18 ng/ml,0.91至3.85)。在区分未感染患者和所有感染患者的受试者工作特征曲线分析中,HMGB1的曲线下面积为0.59(P<0.0001)。HMGB1与白细胞计数、中性粒细胞、C反应蛋白、白细胞介素-6、降钙素原和脂多糖结合蛋白水平仅呈弱相关(P<0.001)。HMGB1与sCD163无相关性。
在一组疑似社区获得性感染和脓毒症的患者中,患者的HMGB1水平与健康对照者相比在统计学上显著更高。感染患者与未感染患者之间无统计学显著差异。HMGB1水平与其他促炎标志物仅呈非常弱的相关性,且与抗炎标志物sCD163无相关性。