Colson Katherine Ellicott, Dwyer-Lindgren Laura, Achoki Tom, Fullman Nancy, Schneider Matthew, Mulenga Peter, Hangoma Peter, Ng Marie, Masiye Felix, Gakidou Emmanuela
University of California, Berkeley (UC Berkeley), Berkeley, CA, USA.
Institute for Health Metrics and Evaluation, University of Washington, Seattle, WA, USA.
BMC Med. 2015 Apr 2;13:69. doi: 10.1186/s12916-015-0308-5.
Achieving universal health coverage and reducing health inequalities are primary goals for an increasing number of health systems worldwide. Timely and accurate measurements of levels and trends in key health indicators at local levels are crucial to assess progress and identify drivers of success and areas that may be lagging behind.
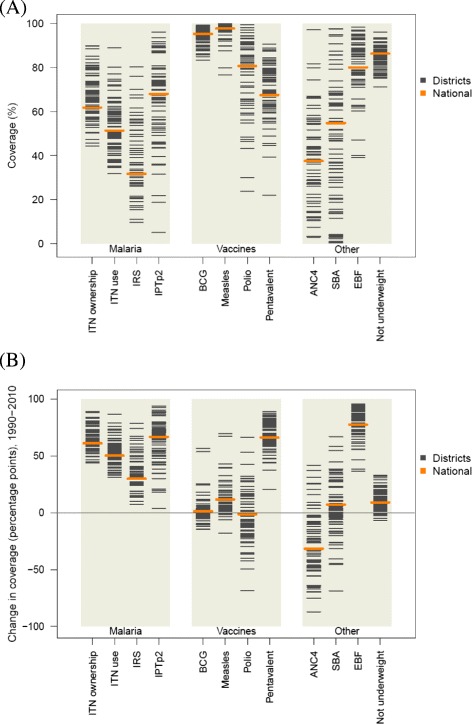
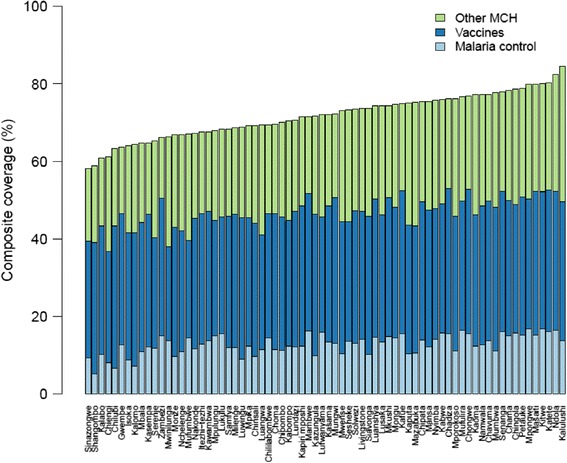
We generated estimates of 17 key maternal and child health indicators for Zambia's 72 districts from 1990 to 2010 using surveys, censuses, and administrative data. We used a three-step statistical model involving spatial-temporal smoothing and Gaussian process regression. We generated estimates at the national level for each indicator by calculating the population-weighted mean of the district values and calculated composite coverage as the average of 10 priority interventions.
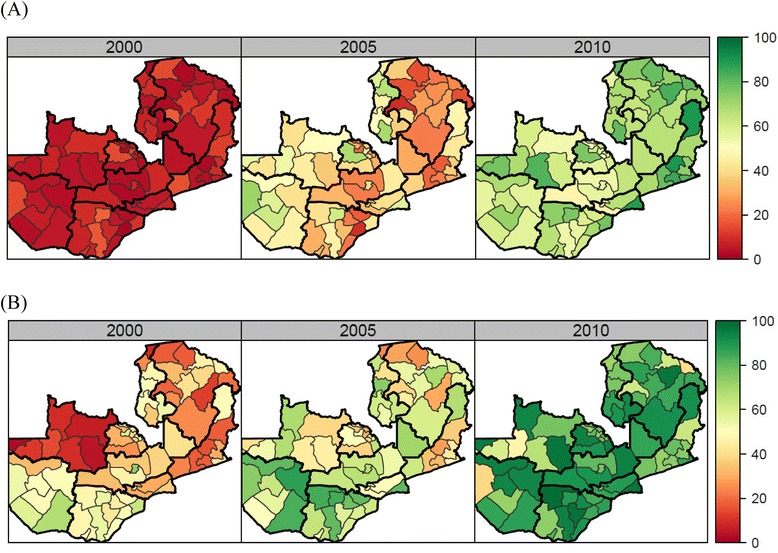
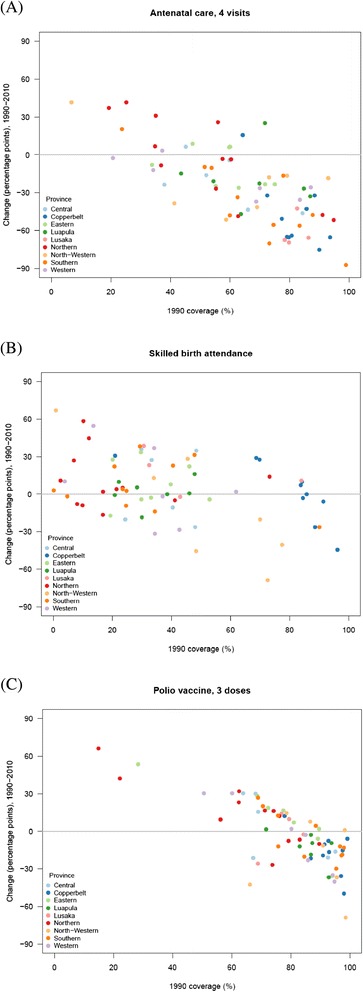
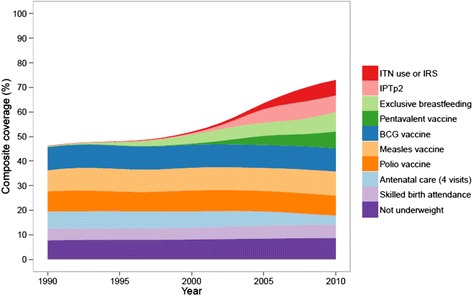
National estimates masked substantial variation across districts in the levels and trends of all indicators. Overall, composite coverage increased from 46% in 1990 to 73% in 2010, and most of this gain was attributable to the scale-up of malaria control interventions, pentavalent immunization, and exclusive breastfeeding. The scale-up of these interventions was relatively equitable across districts. In contrast, progress in routine services, including polio immunization, antenatal care, and skilled birth attendance, stagnated or declined and exhibited large disparities across districts. The absolute difference in composite coverage between the highest-performing and lowest-performing districts declined from 37 to 26 percentage points between 1990 and 2010, although considerable variation in composite coverage across districts persisted.
Zambia has made marked progress in delivering maternal and child health interventions between 1990 and 2010; nevertheless, substantial variations across districts and interventions remained. Subnational benchmarking is important to identify these disparities, allowing policymakers to prioritize areas of greatest need. Analyses such as this one should be conducted regularly and feed directly into policy decisions in order to increase accountability at the local, regional, and national levels.
实现全民健康覆盖和减少健康不平等是全球越来越多卫生系统的首要目标。及时、准确地衡量地方层面关键健康指标的水平和趋势对于评估进展、确定成功驱动因素以及找出可能滞后的领域至关重要。
我们利用调查、人口普查和行政数据,对赞比亚72个地区1990年至2010年的17项关键母婴健康指标进行了估计。我们使用了一个三步统计模型,包括时空平滑和高斯过程回归。我们通过计算各地区数值的人口加权平均值,得出了每个指标在国家层面的估计值,并将综合覆盖率计算为10项优先干预措施的平均值。
国家层面的估计掩盖了各地区所有指标在水平和趋势上的巨大差异。总体而言,综合覆盖率从1990年的46%提高到2010年的73%,这一增长主要归因于疟疾控制干预措施、五价疫苗接种和纯母乳喂养的扩大。这些干预措施的扩大在各地区相对公平。相比之下,包括脊髓灰质炎免疫、产前护理和熟练接生服务在内的常规服务进展停滞或下降,且各地区存在巨大差异。1990年至2010年间,表现最佳和最差地区之间的综合覆盖率绝对差值从37个百分点降至26个百分点,尽管各地区的综合覆盖率仍存在相当大的差异。
赞比亚在1990年至2010年期间提供母婴健康干预措施方面取得了显著进展;然而,各地区和干预措施之间仍存在巨大差异。进行次国家级别的基准评估对于识别这些差异很重要,这使政策制定者能够确定最需要的领域并优先处理。应定期进行此类分析,并将其直接纳入政策决策,以提高地方、区域和国家层面的问责制。