Santiago Marina, Eysenbach Lindsay, Allegretti Jessica, Aroniadis Olga, Brandt Lawrence J, Fischer Monika, Grinspan Ari, Kelly Colleen, Morrow Casey, Rodriguez Martin, Osman Majdi, Kassam Zain, Smith Mark B, Timberlake Sonia
Finch Therapeutics, 200 Inner Belt Rd, Somerville, MA 02143, USA.
OpenBiome, 2067 Massachusetts Ave, Cambridge, MA 02140, USA.
AIMS Microbiol. 2019 Jan 17;5(1):1-18. doi: 10.3934/microbiol.2019.1.1. eCollection 2019.
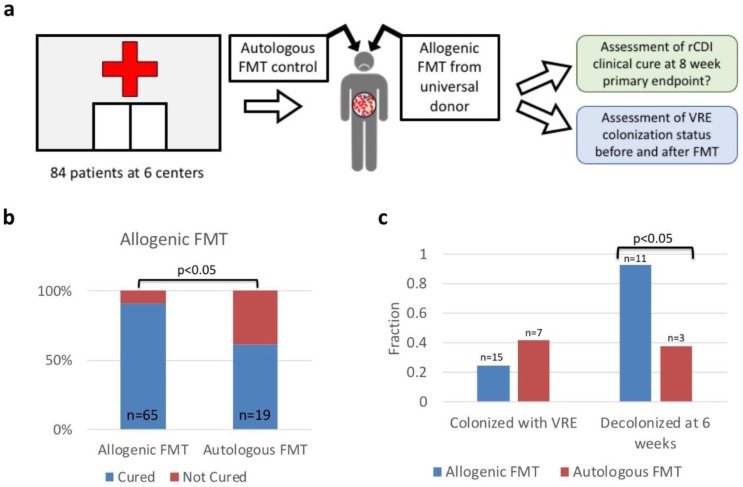
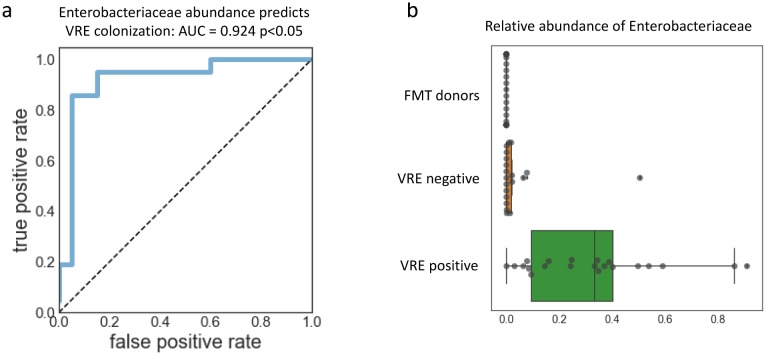
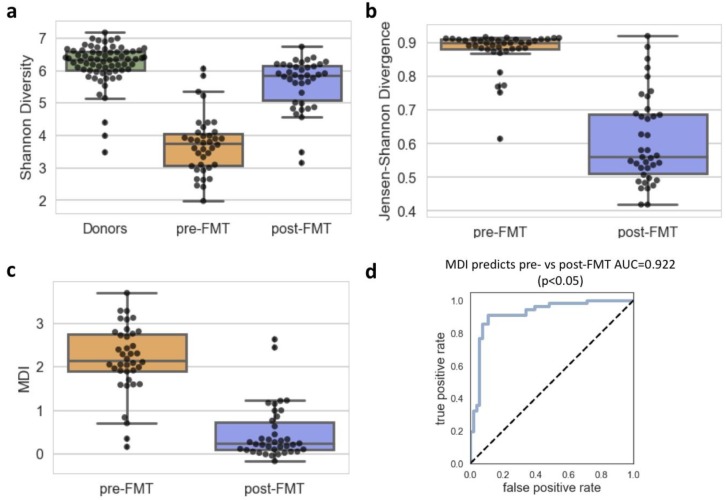
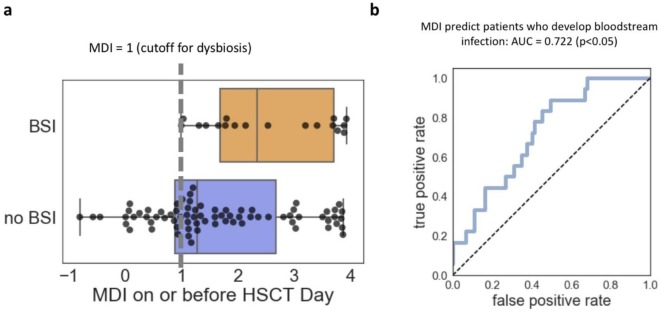
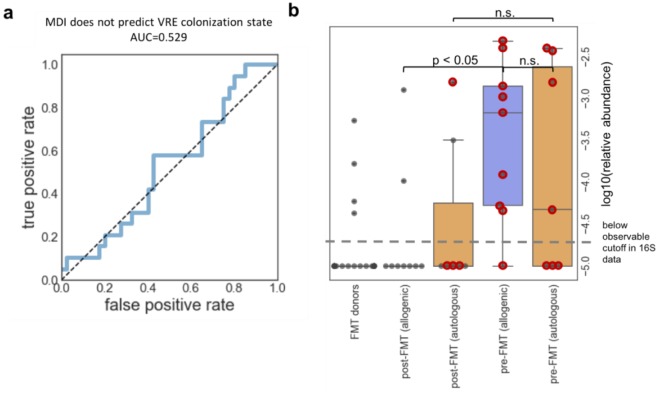
The gastrointestinal microbiome is intrinsically linked to the spread of antibiotic resistance. Antibiotic treatment puts patients at risk for colonization by opportunistic pathogens like vancomycin resistant Enterococcus and by destroying the colonization resistance provided by the commensal microbiota. Once colonized, the host is at a much higher risk for infection by that pathogen. Furthermore, we know that microbiome community differences are associated with disease states, but we do not have a good understanding of how we can use these changes to classify different patient populations. To that end, we have performed a multicenter retrospective analysis on patients who received fecal microbiota transplants to treat recurrent infection. We performed 16S rRNA gene sequencing on fecal samples collected as part of this study and used these data to develop a microbiome disruption index. Our microbiome disruption index is a simple index that is predictive across cohorts, indications, and batch effects. We are able to classify pre-fecal transplant vs post-fecal transplant samples in patients with recurrent infection, and we are able to predict, using previously-published data from a cohort of patients receiving hematopoietic stem cell transplants, which patients would go on to develop bloodstream infections. Finally, we also identified patients in this cohort that were initially colonized with vancomycin resistant Enterococcus and that 92% (11/12) were decolonized after the transplant, but the microbiome disruption index was unable to predict such decolonization. We, however, were able to compare the relative abundance of different taxa between the two groups, and we found that increased abundance of Enterobacteriaceae predicts whether patients were colonized with vancomycin resistant Enterococcus. This work is an early step towards a better understanding of how microbiome predictors can be used to help improve patient care and patient outcomes.
胃肠道微生物群与抗生素耐药性的传播有着内在联系。抗生素治疗会使患者面临被机会性病原体(如耐万古霉素肠球菌)定植的风险,因为它会破坏共生微生物群提供的定植抗性。一旦被定植,宿主被该病原体感染的风险就会高得多。此外,我们知道微生物群落差异与疾病状态有关,但我们对如何利用这些变化来对不同患者群体进行分类还没有很好的理解。为此,我们对接受粪便微生物群移植以治疗复发性感染的患者进行了一项多中心回顾性分析。我们对作为本研究一部分收集的粪便样本进行了16S rRNA基因测序,并利用这些数据开发了一个微生物群破坏指数。我们的微生物群破坏指数是一个简单的指数,在不同队列、适应症和批次效应中都具有预测性。我们能够对复发性感染患者的粪便移植前和移植后样本进行分类,并且能够利用先前发表的一组接受造血干细胞移植患者的数据预测哪些患者会发生血流感染。最后,我们还在这个队列中识别出最初被耐万古霉素肠球菌定植的患者,其中92%(11/12)在移植后被清除定植,但微生物群破坏指数无法预测这种清除定植情况。然而,我们能够比较两组之间不同分类群的相对丰度,并且发现肠杆菌科丰度的增加可以预测患者是否被耐万古霉素肠球菌定植。这项工作是朝着更好地理解如何利用微生物群预测指标来帮助改善患者护理和患者预后迈出的早期一步。