ERA-EDTA Registry, Department of Medical Informatics, Amsterdam Public Health Research Institute, Amsterdam UMC, University of Amsterdam, Amsterdam, The Netherlands.
Deutsche Stiftung Organtransplantation, Frankfurt am Main, Germany.
Nephrol Dial Transplant. 2022 Feb 25;37(3):477-488. doi: 10.1093/ndt/gfab059.
Access to various kidney replacement therapy (KRT) modalities for patients with end-stage kidney disease differs substantially within Europe.
European adults on KRT filled out an online or paper-based survey about factors influencing and experiences with modality choice (e.g. information provision, decision-making and reasons for choice) between November 2017 and January 2019. We compared countries with low, middle and high gross domestic product (GDP).
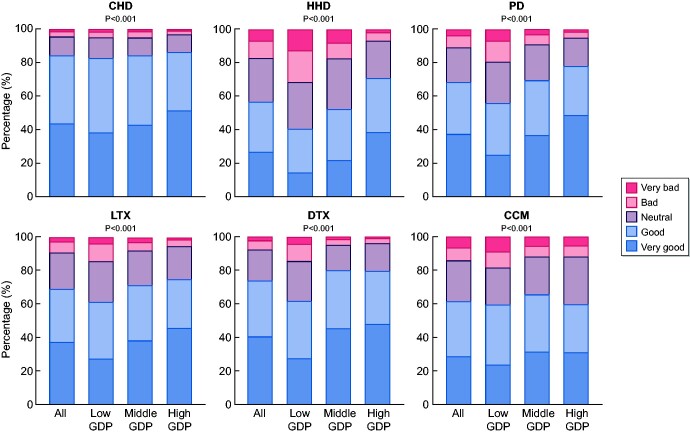
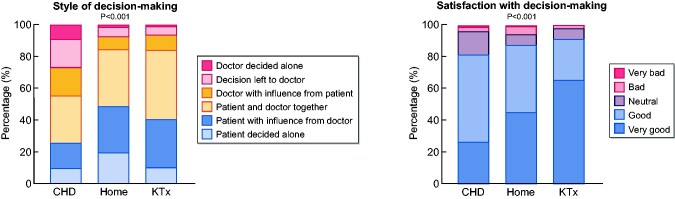
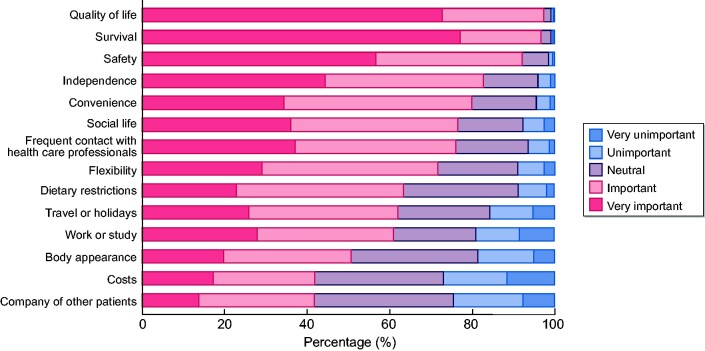
In total, 7820 patients [mean age 59 years, 56% male, 63% on centre haemodialysis (CHD)] from 38 countries participated. Twenty-five percent had received no information on the different modalities, and only 23% received information >12 months before KRT initiation. Patients were not informed about home haemodialysis (HHD) (42%) and comprehensive conservative management (33%). Besides nephrologists, nurses more frequently provided information in high-GDP countries, whereas physicians other than nephrologists did so in low-GDP countries. Patients from low-GDP countries reported later information provision, less information about other modalities than CHD and lower satisfaction with information. The majority of modality decisions were made involving both patient and nephrologist. Patients reported subjective (e.g. quality of life and fears) and objective reasons (e.g. costs and availability of treatments) for modality choice. Patients had good experiences with all modalities, but experiences were better for HHD and kidney transplantation and in middle- and high-GDP countries.
Our results suggest European differences in patient-reported factors influencing KRT modality choice, possibly caused by disparities in availability of KRT modalities, different healthcare systems and varying patient preferences. Availability of home dialysis and kidney transplantation should be optimized.
在欧洲,终末期肾病患者获得各种肾脏替代疗法(KRT)的方式存在很大差异。
2017 年 11 月至 2019 年 1 月,欧洲接受 KRT 的成年人在线或填写纸质问卷,内容为影响和体验 KRT 方式选择的因素(例如信息提供、决策和选择原因)。我们比较了低、中、高国内生产总值(GDP)的国家。
共有来自 38 个国家的 7820 名患者(平均年龄 59 岁,56%为男性,63%接受中心血液透析(CHD))参与了这项研究。25%的患者没有收到关于不同方式的信息,只有 23%的患者在开始 KRT 前 12 个月以上收到信息。患者未被告知家庭血液透析(HHD)(42%)和全面保守治疗(33%)。在高 GDP 国家,护士比医生更频繁地提供信息,而在低 GDP 国家,除了肾病医生之外的医生也会提供信息。低 GDP 国家的患者报告说信息提供时间较晚,有关 CHD 以外其他方式的信息较少,对信息的满意度较低。大多数方式决策都涉及患者和肾病医生。患者报告了选择方式的主观(例如生活质量和恐惧)和客观原因(例如成本和治疗方法的可用性)。患者对所有方式都有较好的体验,但在 HHD 和肾移植以及中高 GDP 国家的体验更好。
我们的研究结果表明,欧洲在影响 KRT 方式选择的患者报告因素方面存在差异,这可能是由于 KRT 方式的可及性、不同的医疗保健系统和不同的患者偏好造成的。应优化家庭透析和肾移植的可及性。