Department of Endocrinology, Amsterdam University Medical Center, Academic Medical Center, Amsterdam, the Netherlands.
Endocrinol Metab (Seoul). 2021 Oct;36(5):938-951. doi: 10.3803/EnM.2021.501. Epub 2021 Sep 30.
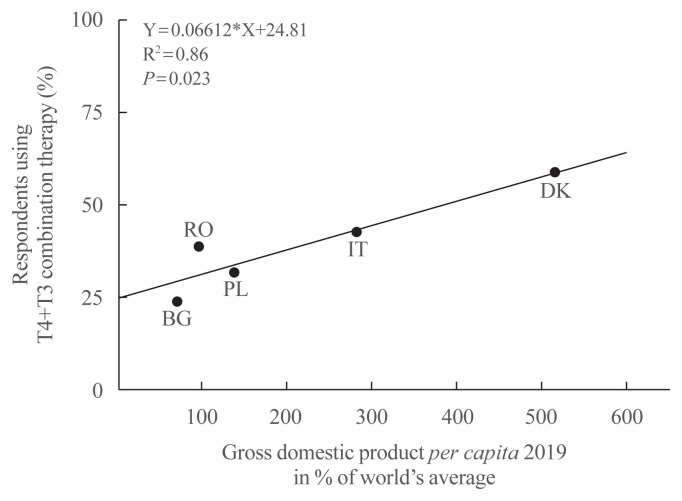
Thyroxine (T4)+triiodothyronine (T3) combination therapy can be considered in case of persistent symptoms despite normal serum thyroid stimulating hormone in levothyroxine (LT4)-treated hypothyroid patients. Combination therapy has gained popularity in the last two decades, especially in countries with a relatively high gross domestic product. The prevalence of persistent symptoms has also increased; most frequent are complaints about energy levels and fatigue (80% to 90%), weight management (70% to 75%), memory (60% to 80%), and mood (40% to 50%). Pathophysiological explanations for persistent problems are unrealistic patient expectations, comorbidities, somatic symptoms, related disorders (Diagnostic and Statistical Manual of Mental Disorders [DSM-5]), autoimmune neuroinflammation, and low tissue T3. There is fair circumstantial evidence for the latter cause (tissue and specifically brain T3 content is normalized by T4+T3, not by T4 alone), but the other causes are viewed as more relevant in current practice. This might be related to the 'hype' that has emerged surrounding T4+T3 therapy. Although more and better-designed trials are needed to validate the efficacy of T4+T3 combination, the management of persistent symptoms should also be directed towards alternative causes. Improving the doctor-patient relationship and including more and better information is crucial. For example, dissatisfaction with the outcomes of T4 treatment for subclinical hypothyroidism can be anticipated as recent trials have demonstrated that LT4 is hardly effective in improving symptoms associated with subclinical hypothyroidism.
尽管甲状腺刺激素(TSH)在左甲状腺素(LT4)治疗的甲状腺功能减退症患者中处于正常范围,但对于持续存在症状的患者,可考虑使用甲状腺素(T4)+三碘甲状腺原氨酸(T3)联合治疗。在过去的二十年中,联合治疗越来越受欢迎,尤其是在国内生产总值相对较高的国家。持续存在症状的患病率也有所增加;最常见的是关于能量水平和疲劳(80%至 90%)、体重管理(70%至 75%)、记忆力(60%至 80%)和情绪(40%至 50%)的抱怨。持续存在问题的病理生理学解释包括不切实际的患者期望、合并症、躯体症状、相关疾病(精神障碍诊断与统计手册第五版[DSM-5])、自身免疫性神经炎症和组织 T3 水平低。后者的原因有一定的间接证据(T4+T3 可使组织 T3 恢复正常,而非仅 T4),但在当前实践中,其他原因被认为更为相关。这可能与 T4+T3 治疗相关的“炒作”有关。尽管需要更多更好设计的试验来验证 T4+T3 联合治疗的疗效,但对于持续存在的症状,也应针对其他原因进行治疗。改善医患关系并提供更多更好的信息至关重要。例如,由于最近的试验表明 LT4 几乎不能有效改善亚临床甲状腺功能减退症相关症状,因此可以预期对亚临床甲状腺功能减退症患者接受 LT4 治疗结局的不满。