Department of Surgery and Cancer, Imperial College London, London.
Department of Acute Medicine, Nottingham University Hospitals NHS Trust, Queen's Medical Centre, Nottingham.
Br J Gen Pract. 2021 Oct 28;71(712):e815-e825. doi: 10.3399/BJGP.2021.0265. Print 2021 Nov.
In the absence of research into therapies and care pathways for long COVID, guidance based on 'emerging experience' is needed.
To provide a rapid expert guide for GPs and long COVID clinical services.
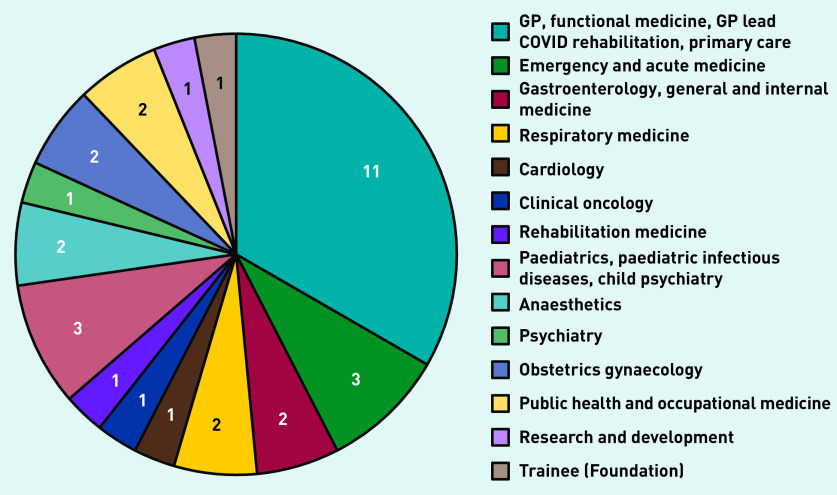
A Delphi study was conducted with a panel of primary and secondary care doctors.
Recommendations were generated relating to the investigation and management of long COVID. These were distributed online to a panel of UK doctors (any specialty) with an interest in, lived experience of, and/or experience treating long COVID. Over two rounds of Delphi testing, panellists indicated their agreement with each recommendation (using a five-point Likert scale) and provided comments. Recommendations eliciting a response of 'strongly agree', 'agree', or 'neither agree nor disagree' from 90% or more of responders were taken as showing consensus.
Thirty-three clinicians representing 14 specialties reached consensus on 35 recommendations. Chiefly, GPs should consider long COVID in the presence of a wide range of presenting features (not limited to fatigue and breathlessness) and exclude differential diagnoses where appropriate. Detailed history and examination with baseline investigations should be conducted in primary care. Indications for further investigation and specific therapies (for myocarditis, postural tachycardia syndrome, mast cell disorder) include hypoxia/desaturation, chest pain, palpitations, and histamine-related symptoms. Rehabilitation should be individualised, with careful activity pacing (to avoid relapse) and multidisciplinary support.
Long COVID clinics should operate as part of an integrated care system, with GPs playing a key role in the multidisciplinary team. Holistic care pathways, investigation of specific complications, management of potential symptom clusters, and tailored rehabilitation are needed.
由于缺乏针对长新冠的治疗方法和护理途径的研究,因此需要基于“新兴经验”提供指导。
为全科医生和长新冠临床服务提供快速的专家指南。
采用德尔菲研究法,对初级和二级保健医生小组进行研究。
针对长新冠的调查和管理,生成了相关建议。这些建议在线分发给对长新冠有兴趣、有亲身经历或有治疗经验的英国医生(任何专业)。在两轮德尔菲测试中,小组成员使用五点李克特量表表示对每条建议的同意程度(表示同意、较同意、不确定、较不同意、不同意),并提供意见。如果 90%或更多的应答者对某条建议的回答是“非常同意”、“同意”或“不确定”,则认为该建议达成共识。
33 名代表 14 个专业的临床医生就 35 条建议达成共识。主要的是,全科医生应考虑到广泛的临床表现(不仅限于疲劳和呼吸困难)出现时存在长新冠,并在适当情况下排除鉴别诊断。在初级保健中应进行详细的病史和体格检查,并进行基线调查。进一步调查和特定治疗(如心肌炎、体位性心动过速综合征、肥大细胞疾病)的指征包括缺氧/低氧血症、胸痛、心悸和与组胺相关的症状。康复应该个体化,进行仔细的活动节奏控制(以避免复发)和多学科支持。
长新冠诊所应该作为综合护理系统的一部分运作,全科医生在多学科团队中发挥关键作用。需要制定整体护理途径、调查特定并发症、管理潜在症状群,并进行针对性康复。