MMWR Morb Mortal Wkly Rep. 2020 Nov 13;69(45):1681-1685. doi: 10.15585/mmwr.mm6945a4.
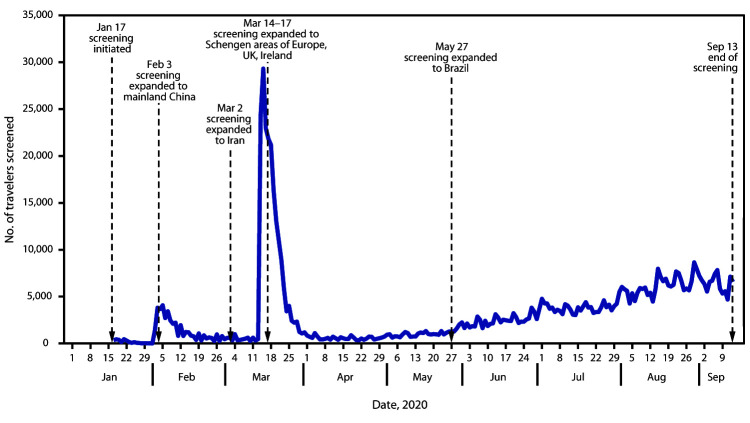
In January 2020, with support from the U.S. Department of Homeland Security (DHS), CDC instituted an enhanced entry risk assessment and management (screening) program for air passengers arriving from certain countries with widespread, sustained transmission of SARS-CoV-2, the virus that causes coronavirus disease 2019 (COVID-19). The objectives of the screening program were to reduce the importation of COVID-19 cases into the United States and slow subsequent spread within states. Screening aimed to identify travelers with COVID-19-like illness or who had a known exposure to a person with COVID-19 and separate them from others. Screening also aimed to inform all screened travelers about self-monitoring and other recommendations to prevent disease spread and obtain their contact information to share with public health authorities in destination states. CDC delegated postarrival management of crew members to airline occupational health programs by issuing joint guidance with the Federal Aviation Administration.* During January 17-September 13, 2020, a total of 766,044 travelers were screened, 298 (0.04%) of whom met criteria for public health assessment; 35 (0.005%) were tested for SARS-CoV-2, and nine (0.001%) had a positive test result. CDC shared contact information with states for approximately 68% of screened travelers because of data collection challenges and some states' opting out of receiving data. The low case detection rate of this resource-intensive program highlighted the need for fundamental change in the U.S. border health strategy. Because SARS-CoV-2 infection and transmission can occur in the absence of symptoms and because the symptoms of COVID-19 are nonspecific, symptom-based screening programs are ineffective for case detection. Since the screening program ended on September 14, 2020, efforts to reduce COVID-19 importation have focused on enhancing communications with travelers to promote recommended preventive measures, reinforcing mechanisms to refer overtly ill travelers to CDC, and enhancing public health response capacity at ports of entry. More efficient collection of contact information for international air passengers before arrival and real-time transfer of data to U.S. health departments would facilitate timely postarrival public health management, including contact tracing, when indicated. Incorporating health attestations, predeparture and postarrival testing, and a period of limited movement after higher-risk travel, might reduce risk for transmission during travel and translocation of SARS-CoV-2 between geographic areas and help guide more individualized postarrival recommendations.
2020 年 1 月,在美国国土安全部(DHS)的支持下,CDC 针对来自广泛、持续传播 SARS-CoV-2 的某些国家的航空旅客实施了入境风险评估和管理(筛查)计划,SARS-CoV-2 是导致 2019 年冠状病毒病(COVID-19)的病毒。该筛查计划的目的是减少 COVID-19 病例输入美国,并减缓各州内的后续传播。筛查旨在识别有 COVID-19 样疾病的旅行者,或有已知与 COVID-19 患者接触的旅行者,并将他们与其他人分开。筛查还旨在向所有接受筛查的旅行者通报自我监测和其他建议,以防止疾病传播,并获取他们的联系信息,以便与目的地州的公共卫生当局共享。CDC 通过与联邦航空管理局联合发布指导意见,将机组人员的抵达后管理委托给航空公司的职业健康计划。*2020 年 1 月 17 日至 9 月 13 日,共有 766,044 名旅客接受了筛查,其中 298 人(0.04%)符合公共卫生评估标准;35 人(0.005%)接受了 SARS-CoV-2 检测,9 人(0.001%)检测结果呈阳性。由于数据收集挑战和一些州选择不接收数据,CDC 与各州共享了大约 68%的筛查旅行者的联系信息。该资源密集型计划的低病例检出率突出表明,美国边境卫生战略需要根本改变。由于 SARS-CoV-2 感染和传播可能在无症状时发生,并且 COVID-19 的症状是非特异性的,因此基于症状的筛查计划对病例检测无效。自 2020 年 9 月 14 日筛查计划结束以来,减少 COVID-19 输入的努力重点是加强与旅行者的沟通,以促进建议的预防措施,加强将明显患病的旅行者转介给 CDC 的机制,并增强入境口岸的公共卫生应对能力。在抵达前更有效地收集国际航空旅客的联系信息,并实时将数据传输到美国卫生部门,将有助于在需要时及时进行抵达后公共卫生管理,包括接触者追踪。纳入健康声明、出发前和抵达后检测以及高风险旅行后的有限活动期,可能会降低旅行期间的传播风险,并有助于在地理区域之间转移 SARS-CoV-2 ,并帮助指导更个性化的抵达后建议。