Department of General Neurosurgery, Center for Neurosurgery, Faculty of Medicine and University Hospital Cologne, University of Cologne, Cologne, Germany.
Department of Neuropathology, Otto-von-Guericke University, Magdeburg, Germany.
Acta Neuropathol Commun. 2022 Aug 6;10(1):109. doi: 10.1186/s40478-022-01411-x.
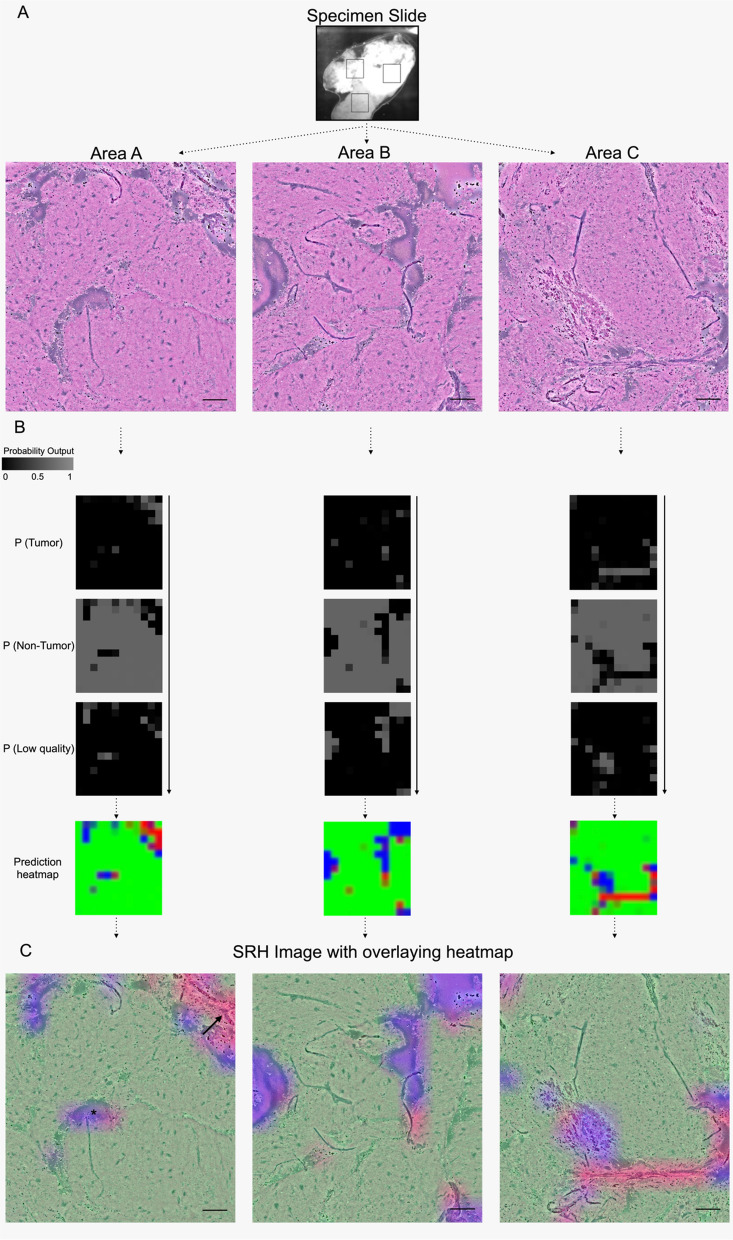
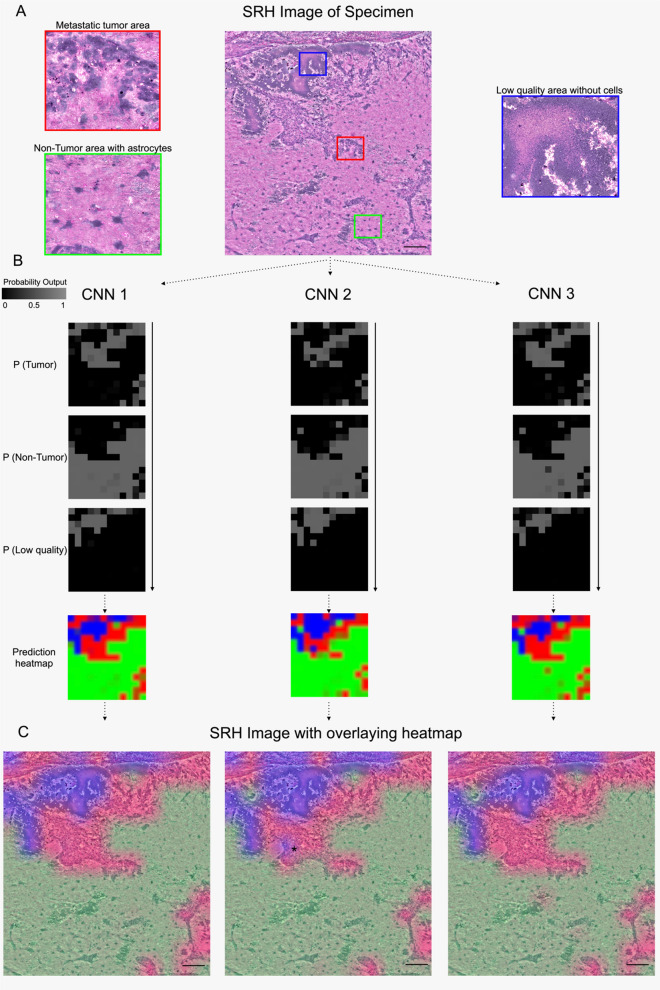
Determining the presence of tumor in biopsies and the decision-making during resections is often dependent on intraoperative rapid frozen-section histopathology. Recently, stimulated Raman scattering microscopy has been introduced to rapidly generate digital hematoxylin-and-eosin-stained-like images (stimulated Raman histology) for intraoperative analysis. To enable intraoperative prediction of tumor presence, we aimed to develop a new deep residual convolutional neural network in an automated pipeline and tested its validity. In a monocentric prospective clinical study with 94 patients undergoing biopsy, brain or spinal tumor resection, Stimulated Raman histology images of intraoperative tissue samples were obtained using a fiber-laser-based stimulated Raman scattering microscope. A residual network was established and trained in ResNetV50 to predict three classes for each image: (1) tumor, (2) non-tumor, and (3) low-quality. The residual network was validated on images obtained in three small random areas within the tissue samples and were blindly independently reviewed by a neuropathologist as ground truth. 402 images derived from 132 tissue samples were analyzed representing the entire spectrum of neurooncological surgery. The automated workflow took in a mean of 240 s per case, and the residual network correctly classified tumor (305/326), non-tumorous tissue (49/67), and low-quality (6/9) images with an inter-rater agreement of 89.6% (κ = 0.671). An excellent internal consistency was found among the random areas with 90.2% (Cα = 0.942) accuracy. In conclusion, the novel stimulated Raman histology-based residual network can reliably detect the microscopic presence of tumor and differentiate from non-tumorous brain tissue in resection and biopsy samples within 4 min and may pave a promising way for an alternative rapid intraoperative histopathological decision-making tool.
在活检中确定肿瘤的存在以及在切除过程中的决策通常依赖于术中快速冷冻切片组织病理学检查。最近,受激拉曼散射显微镜已被引入,以快速生成用于术中分析的数字苏木精-伊红染色样图像(受激拉曼组织学)。为了能够在术中预测肿瘤的存在,我们旨在开发一个新的深度残差卷积神经网络,并在自动流水线中进行测试。在一项 94 例接受活检、脑或脊髓肿瘤切除的患者的单中心前瞻性临床研究中,使用基于光纤激光的受激拉曼散射显微镜获取术中组织样本的受激拉曼组织学图像。建立了一个残差网络,并在 ResNetV50 中进行训练,以对每张图像预测三个类别:(1)肿瘤,(2)非肿瘤,和(3)低质量。该残差网络在组织样本内三个小随机区域获得的图像上进行验证,并由神经病理学家作为金标准进行盲法独立审查。共分析了来自 132 个组织样本的 402 张图像,代表了神经肿瘤学手术的整个范围。自动化工作流程平均每例耗时 240 秒,该残差网络正确分类了肿瘤(305/326)、非肿瘤组织(49/67)和低质量(6/9)图像,观察者间的一致性为 89.6%(κ=0.671)。在随机区域内发现了极好的内部一致性,准确率为 90.2%(Cα=0.942)。总之,新型基于受激拉曼组织学的残差网络可以可靠地检测肿瘤的微观存在,并在 4 分钟内从切除和活检样本中的非肿瘤脑组织中区分开来,可能为替代快速术中组织病理学决策工具铺平道路。