Department of Radiation Physics, University of Texas MD Anderson Cancer Center, Houston, Texas.
Department of Radiation Oncology, Stanford University, Palo Alto, California.
Int J Radiat Oncol Biol Phys. 2021 Mar 1;109(3):801-812. doi: 10.1016/j.ijrobp.2020.10.005. Epub 2020 Oct 14.
To develop a deep learning model that generates consistent, high-quality lymph node clinical target volumes (CTV) contours for head and neck cancer (HNC) patients, as an integral part of a fully automated radiation treatment planning workflow.
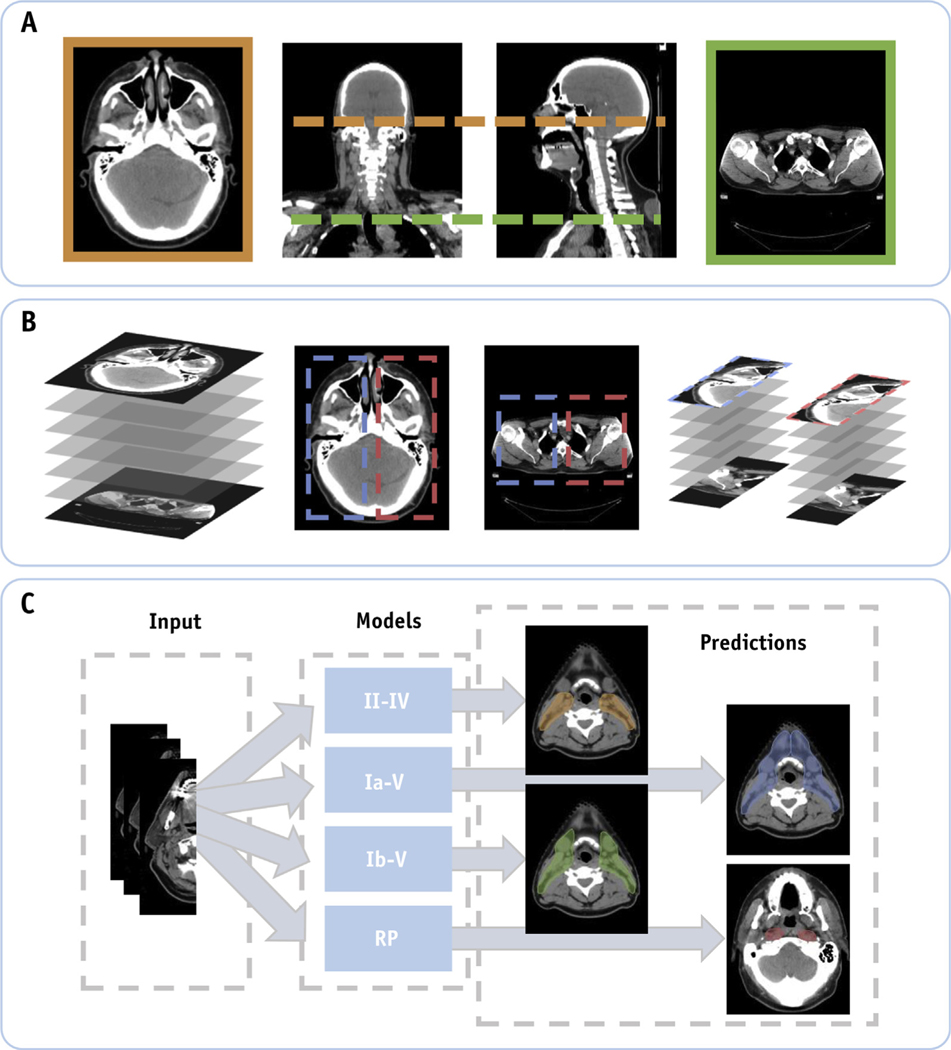
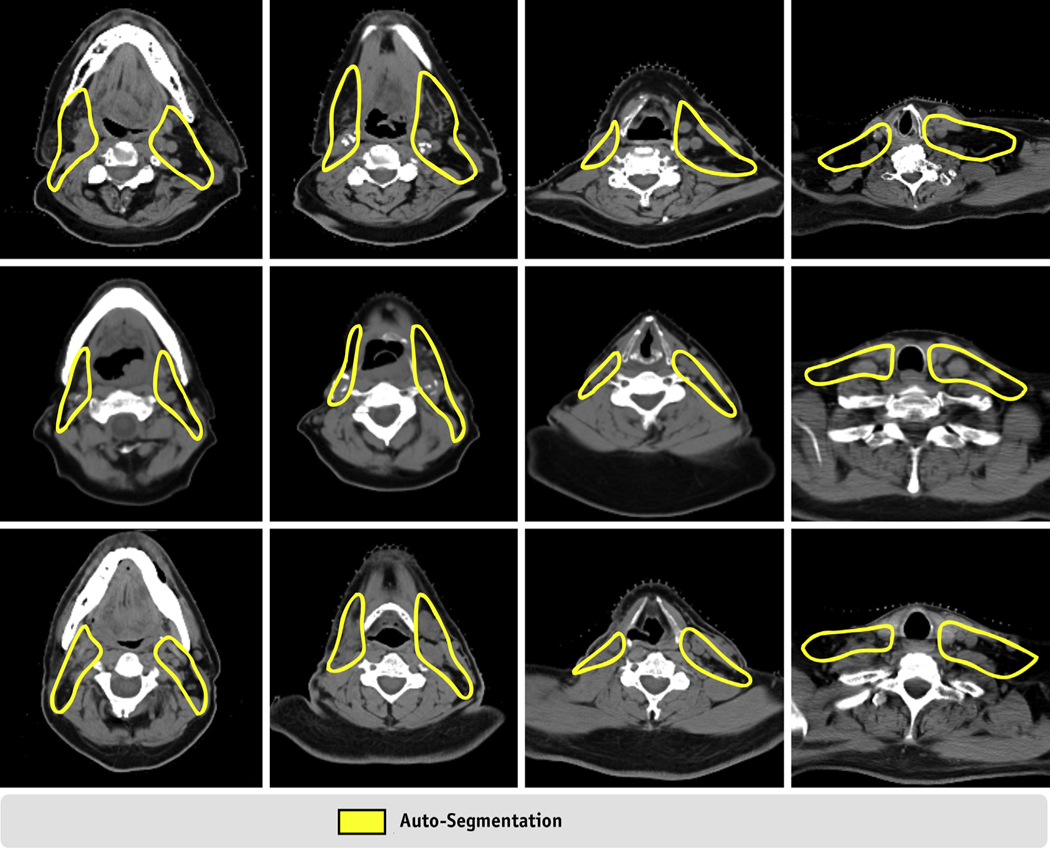
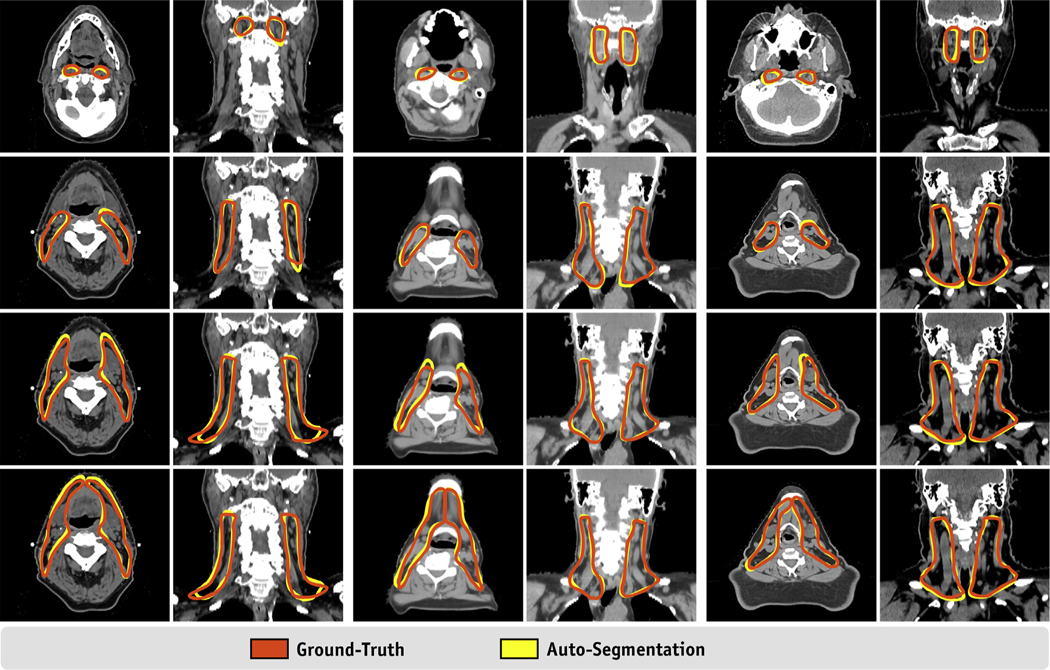
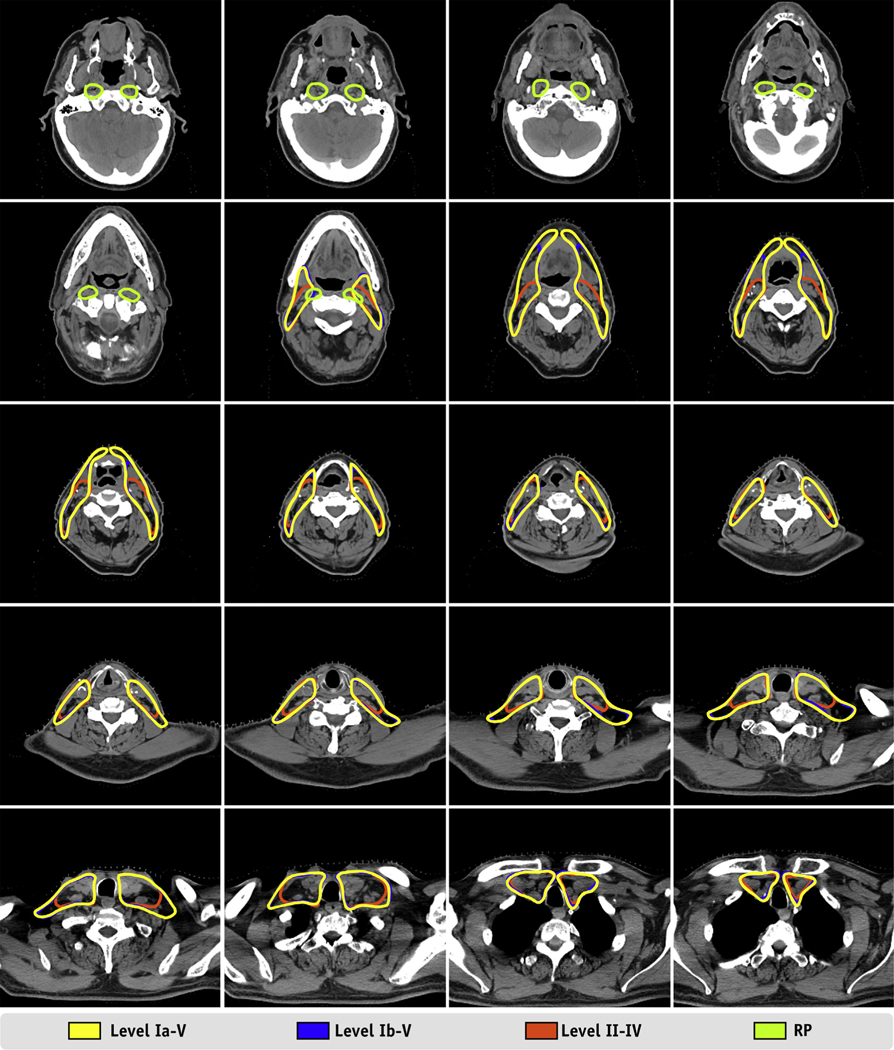
Computed tomography (CT) scans from 71 HNC patients were retrospectively collected and split into training (n = 51), cross-validation (n = 10), and test (n = 10) data sets. All had target volume delineations covering lymph node levels Ia through V (Ia-V), Ib through V (Ib-V), II through IV (II-IV), and retropharyngeal (RP) nodes, which were previously approved by a radiation oncologist specializing in HNC. Volumes of interest (VOIs) about nodal levels were automatically identified using computer vision techniques. The VOI (cropped CT image) and approved contours were used to train a U-Net autosegmentation model. Each lymph node level was trained independently, with model parameters optimized by assessing performance on the cross-validation data set. Once optimal model parameters were identified, overlap and distance metrics were calculated between ground truth and autosegmentations on the test set. Lastly, this final model was used on 32 additional patient scans (not included in original 71 cases) and autosegmentations visually rated by 3 radiation oncologists as being "clinically acceptable without requiring edits," "requiring minor edits," or "requiring major edits."
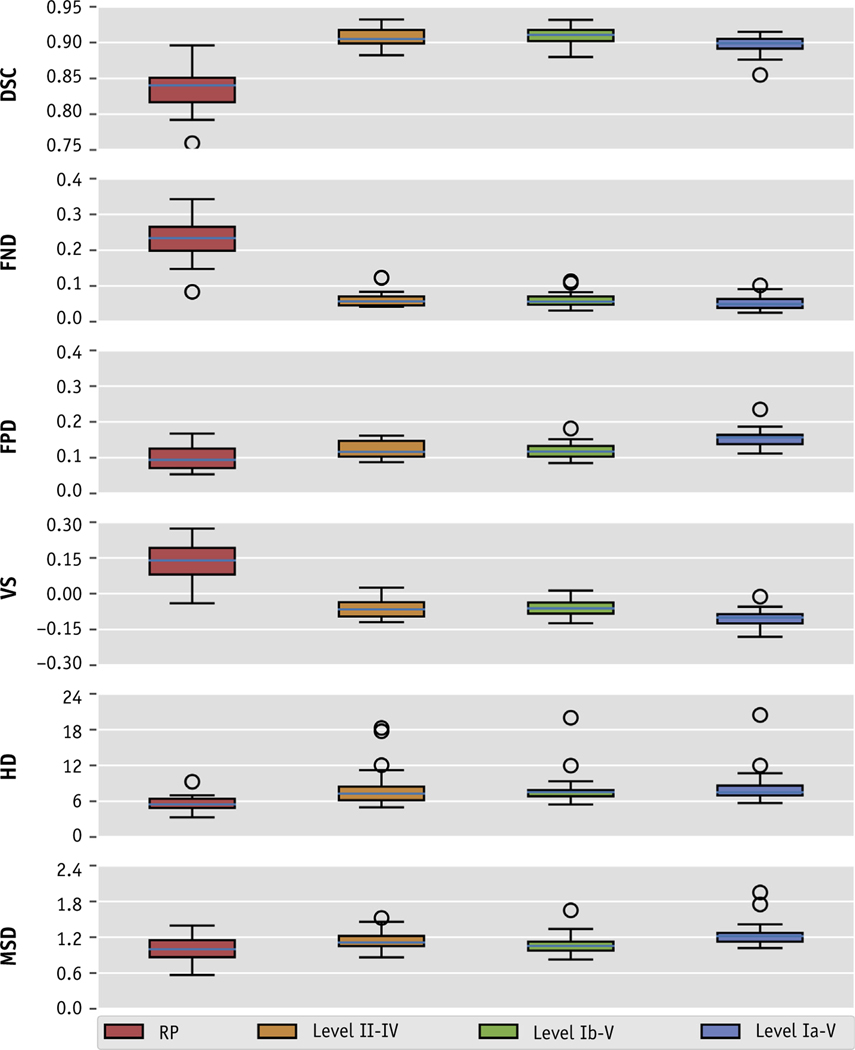
When comparing ground truths to autosegmentations on the test data set, median Dice Similarity Coefficients were 0.90, 0.90, 0.89, and 0.81, and median mean surface distance values were 1.0 mm, 1.0 mm, 1.1 mm, and 1.3 mm for node levels Ia-V, Ib-V, II-IV, and RP nodes, respectively. Qualitative scoring varied among physicians. Overall, 99% of autosegmented target volumes were either scored as being clinically acceptable or requiring minor edits (ie, stylistic recommendations, <2 minutes).
We developed a fully automated artificial intelligence approach to autodelineate nodal CTVs for patients with intact HNC. Most autosegmentations were found to be clinically acceptable after qualitative review when considering recommended stylistic edits. This promising work automatically delineates nodal CTVs in a robust and consistent manner; this approach can be implemented in ongoing efforts for fully automated radiation treatment planning.
开发一种深度学习模型,为头颈部癌症(HNC)患者生成一致、高质量的淋巴结临床靶区(CTV)轮廓,作为全自动放射治疗计划工作流程的一个组成部分。
回顾性收集了 71 例 HNC 患者的计算机断层扫描(CT)扫描,并将其分为训练集(n=51)、交叉验证集(n=10)和测试集(n=10)。所有患者的靶区均涵盖淋巴结水平 Ia 至 V(Ia-V)、Ib 至 V(Ib-V)、II 至 IV(II-IV)和咽后(RP)区域,这些区域的勾画均由专门从事 HNC 的放射肿瘤学家预先批准。使用计算机视觉技术自动识别感兴趣的体积(VOI)。使用 VOI(裁剪后的 CT 图像)和批准的轮廓来训练 U-Net 自动分割模型。每个淋巴结水平都是独立训练的,通过在交叉验证数据集上评估性能来优化模型参数。一旦确定了最佳模型参数,就在测试集上计算真实值和自动分割之间的重叠和距离度量。最后,将这个最终模型应用于 32 例额外的患者扫描(不包括原始 71 例中的患者),并由 3 名放射肿瘤学家对自动勾画进行视觉评估,判断是否“无需编辑即可临床接受”、“需要少量编辑”或“需要大量编辑”。
在测试数据集上,将真实值与自动分割进行比较,Ia-V、Ib-V、II-IV 和 RP 淋巴结的中位 Dice 相似系数分别为 0.90、0.90、0.89 和 0.81,中位平均表面距离值分别为 1.0mm、1.0mm、1.1mm 和 1.3mm。医生之间的定性评分存在差异。总体而言,99%的目标体积自动勾画被评为临床可接受或仅需少量编辑(即风格建议,<2 分钟)。
我们开发了一种全自动人工智能方法,用于自动勾画完整 HNC 患者的淋巴结 CTV。在考虑推荐的风格编辑后,通过定性审查,大多数自动勾画被认为是临床可接受的。这项有前途的工作以稳健且一致的方式自动勾画淋巴结 CTV;这种方法可以应用于全自动放射治疗计划的持续努力中。